

Magnetic Resonance Imaging-Based Prediction of the Relationship between Whiplash Injury and Temporomandibular Disorders
- PMID: 29375466
- PMCID: PMC5767220
- DOI: 10.3389/fneur.2017.00725
Magnetic Resonance Imaging-Based Prediction of the Relationship between Whiplash Injury and Temporomandibular Disorders
Abstract
Purpose: Whiplash injury can cause internal derangement of the temporomandibular joint (TMJ) and lead to temporomandibular disorders (TMDs). Our aim was to evaluate whether the initial clinical findings in TMD patients with whiplash injury are correlated with their magnetic resonance imaging (MRI) characteristics.
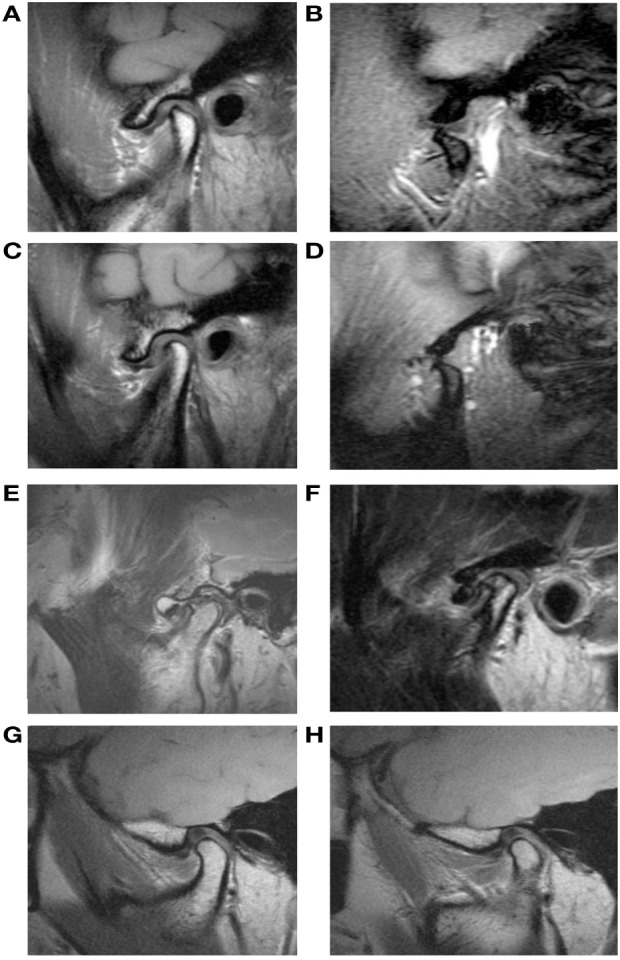
Materials and methods: This case-control study involved 219 patients (135 women, 84 men; mean age: 37.84 years) who visited our orofacial pain clinic with TMD; TMD was diagnosed using the diagnostic criteria for TMD Axis I. Patients were categorized into three groups based on the presence and type of macrotrauma: in the "wTMD" group, patients had suffered whiplash injury; patients in the "pTMD" group had post-traumatic TMD; the "iTMD" group comprised patients who had presented with TMD symptoms and had sustained no macrotrauma. We investigated the presence of disk displacement, effusion, disk deformity, and condylar degeneration, and changes in the lateral pterygoid muscle (LPM). To evaluate the severity of TMD pain and objectively analyze symptoms, we used a visual analog scale (VAS), palpation index (PI), neck PI, dysfunction index, and craniomandibular index (CMI).
Results: The VAS scores, and the severity indexes of the TMD including PI, neck PI, and CMI were highest in the wTMD patients. Atrophy of the LPM was most commonly seen in the wTMD group, as was disk deformity. In wTMD patients only, VAS score was significantly correlated with stress; it was correlated with headache in wTMD and iTMD patients. The clinical symptoms of TMD were not correlated with MRI findings in the wTMD group. However, alterations in the LPM were strongly correlated with disk displacement.
Conclusion: If clinicians recognize alterations in the LPM and disk displacement in the TMJ, they will better understand the clinical symptoms and pathophysiology of TMD with whiplash injury. Whiplash injury may lead to TMD via different mechanisms from other macrotraumas.
Keywords: macrotrauma; magnetic resonance imaging; neck pain; temporomandibular disorder; whiplash injury.
Figures
Similar articles
-
MRI-Based Assessment of Masticatory Muscle Changes in TMD Patients after Whiplash Injury.J Clin Med. 2021 Apr 1;10(7):1404. doi: 10.3390/jcm10071404. J Clin Med. 2021. PMID: 33915742 Free PMC article.
-
Sex-related differences in symptoms of temporomandibular disorders and structural changes in the lateral pterygoid muscle after whiplash injury.J Oral Rehabil. 2019 Dec;46(12):1107-1120. doi: 10.1111/joor.12845. Epub 2019 Jul 15. J Oral Rehabil. 2019. PMID: 31228222
-
Evaluation of the lateral pterygoid muscle using magnetic resonance imaging.Dentomaxillofac Radiol. 2010 Dec;39(8):494-500. doi: 10.1259/dmfr/80928433. Dentomaxillofac Radiol. 2010. PMID: 21062943 Free PMC article.
-
Role of magnetic resonance imaging in the clinical diagnosis of the temporomandibular joint.Cells Tissues Organs. 2005;180(1):6-21. doi: 10.1159/000086194. Cells Tissues Organs. 2005. PMID: 16088129 Review.
-
Are Whiplash-Associated Disorders and Temporomandibular Disorders in a Trauma Related Cause and Effect Relationship? A Review.Medicina (Kaunas). 2023 Aug 17;59(8):1482. doi: 10.3390/medicina59081482. Medicina (Kaunas). 2023. PMID: 37629772 Free PMC article. Review.
Cited by
-
Clinical factors affecting depression in patients with painful temporomandibular disorders during the COVID-19 pandemic.Sci Rep. 2022 Aug 29;12(1):14667. doi: 10.1038/s41598-022-18745-0. Sci Rep. 2022. PMID: 36038574 Free PMC article.
-
Automatic detection and visualization of temporomandibular joint effusion with deep neural network.Sci Rep. 2024 Aug 14;14(1):18865. doi: 10.1038/s41598-024-69848-9. Sci Rep. 2024. PMID: 39143180 Free PMC article.
-
Investigation of Snoring and Obstructive Sleep Apnea Using Portable Polysomnography in Patients with Temporomandibular Disorder.Dent Res Oral Health. 2022;5(3):63-73. doi: 10.26502/droh.0050. Epub 2022 Sep 30. Dent Res Oral Health. 2022. PMID: 36276181 Free PMC article.
-
Causal Relationship Between Autoimmune Arthritis and Temporomandibular Disorders.Int Dent J. 2025 Apr;75(2):596-604. doi: 10.1016/j.identj.2024.08.006. Epub 2024 Sep 3. Int Dent J. 2025. PMID: 39232938 Free PMC article.
-
Sleep analysis results of portable polysomnography in patients with acute and chronic temporomandibular disorder.Dent Res Oral Health. 2022;5(4):83-93. doi: 10.26502/droh.0052. Epub 2022 Oct 7. Dent Res Oral Health. 2022. PMID: 36330079 Free PMC article.
References
-
- Spitzer WO, Skovron ML, Salmi LR, Cassidy JD, Duranceau J, Suissa S, et al. Scientific monograph of the Quebec Task Force on Whiplash-Associated Disorders: redefining “whiplash” and its management. Spine (1995) 20:1s–73s. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous