

Blood Gene Expression Predicts Bronchiolitis Obliterans Syndrome
- PMID: 29375549
- PMCID: PMC5768645
- DOI: 10.3389/fimmu.2017.01841
Blood Gene Expression Predicts Bronchiolitis Obliterans Syndrome
Abstract
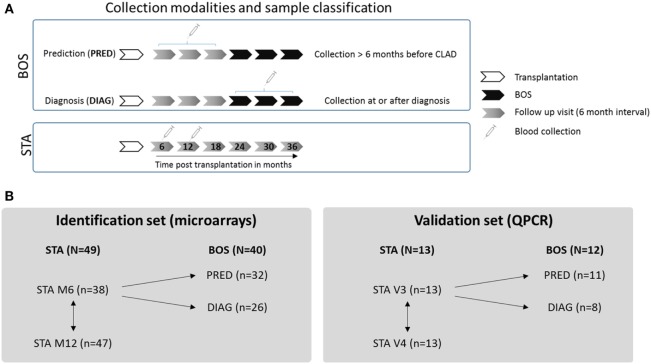
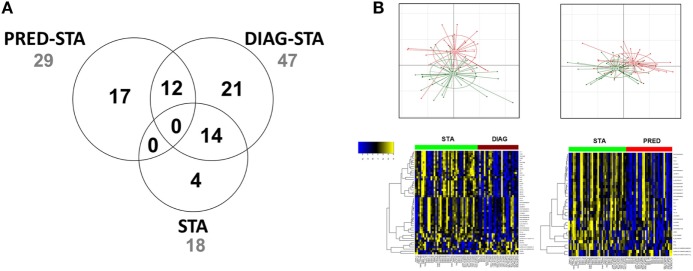
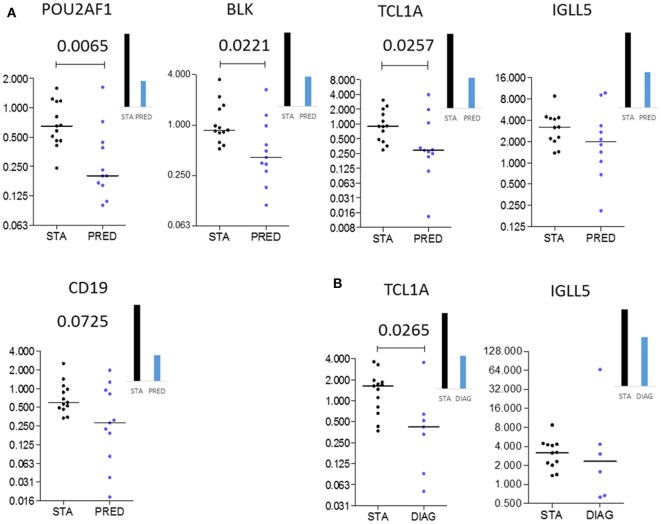
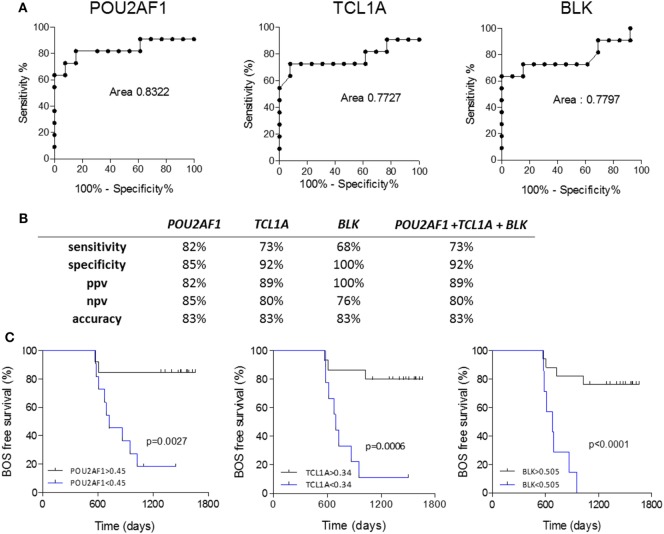
Bronchiolitis obliterans syndrome (BOS), the main manifestation of chronic lung allograft dysfunction, leads to poor long-term survival after lung transplantation. Identifying predictors of BOS is essential to prevent the progression of dysfunction before irreversible damage occurs. By using a large set of 107 samples from lung recipients, we performed microarray gene expression profiling of whole blood to identify early biomarkers of BOS, including samples from 49 patients with stable function for at least 3 years, 32 samples collected at least 6 months before BOS diagnosis (prediction group), and 26 samples at or after BOS diagnosis (diagnosis group). An independent set from 25 lung recipients was used for validation by quantitative PCR (13 stables, 11 in the prediction group, and 8 in the diagnosis group). We identified 50 transcripts differentially expressed between stable and BOS recipients. Three genes, namely POU class 2 associating factor 1 (POU2AF1), T-cell leukemia/lymphoma protein 1A (TCL1A), and B cell lymphocyte kinase, were validated as predictive biomarkers of BOS more than 6 months before diagnosis, with areas under the curve of 0.83, 0.77, and 0.78 respectively. These genes allow stratification based on BOS risk (log-rank test p < 0.01) and are not associated with time posttransplantation. This is the first published large-scale gene expression analysis of blood after lung transplantation. The three-gene blood signature could provide clinicians with new tools to improve follow-up and adapt treatment of patients likely to develop BOS.
Keywords: biomarkers; blood; bronchiolitis obliterans syndrome; gene expression; lung transplantation.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases