

Predictors of Insulin Resistance in Children versus Adolescents with Obesity
- PMID: 29375912
- PMCID: PMC5742469
- DOI: 10.1155/2017/3793868
Predictors of Insulin Resistance in Children versus Adolescents with Obesity
Abstract
Introduction: Obesity is a risk factor to develop metabolic syndrome (MetS) and type 2 diabetes mellitus (T2DM). Insulin resistance (IR) plays a major part in both. With increasing incidence of childhood obesity, this retrospective study aimed to identify predictors of IR in children/adolescents with obesity to optimize screening for IR.
Method: Patients aged ≥ 2-≤ 18 years with obesity (BMI-SDS > 2.3) were included. IR was defined as HOMA-IR ≥ 3.4, and MetS if ≥3 of the following criteria were present: waist circumference and blood pressure ≥ 95th age percentile, triglycerides ≥ 1.7 mmol/l, HDL < 1.03 mmol/l, and fasting plasma glucose ≥ 5.6 mmol/l.
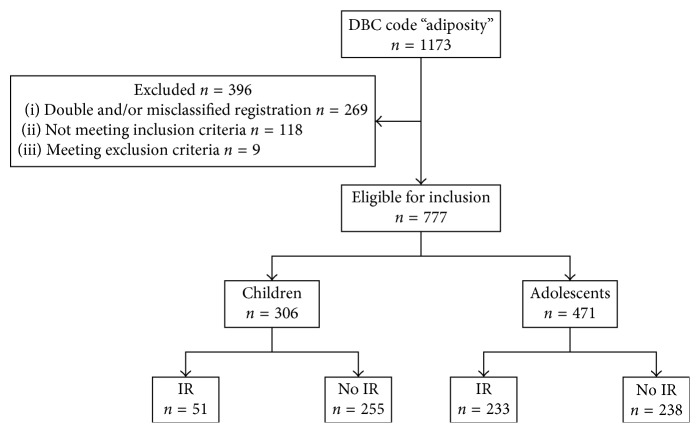
Results: In total, 777 patients were included. Of the 306 children, 51, 38, and 0 were diagnosed with IR, MetS, and T2DM, respectively. Of the 471 adolescents, 223, 95, and 0 were diagnosed with IR, MetS, and T2DM, respectively. In the multivariable regression model, BMI-SDS, preterm birth, and Tanner stage were associated with IR in children (6.3 (95% CI 1.3-31.1), 5.4 (95% CI 1.4-20.5), 2.2 (95% CI 1.0-4.8)), and BMI-SDS and waist circumference in adolescents (4.0 (95% CI 1.7-9.2), 3.7 (95% CI 1.5-9.4)).
Conclusion: Different IR predictors were observed in children/adolescents with obesity. These predictors can be used to optimize screening for IR in pediatric populations.
References
-
- World Health Organisation. Global and regional trends by UN Regions, 1990–2025; Overweight: 1990–2015. June 2016, http://apps.who.int/gho/data/node.main.NUTUNREGIONS?lang=en.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
