

Factors influencing risk-based care of the childhood cancer survivor in the 21st century
- PMID: 29377070
- PMCID: PMC8893118
- DOI: 10.3322/caac.21445
Factors influencing risk-based care of the childhood cancer survivor in the 21st century
Abstract
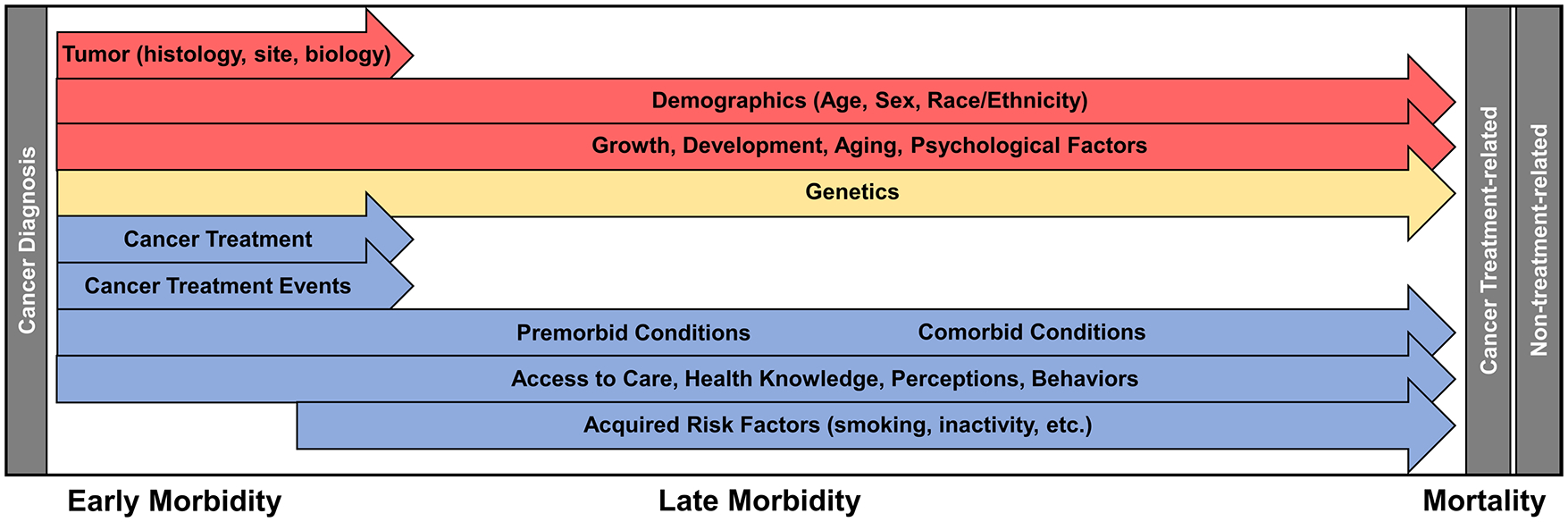
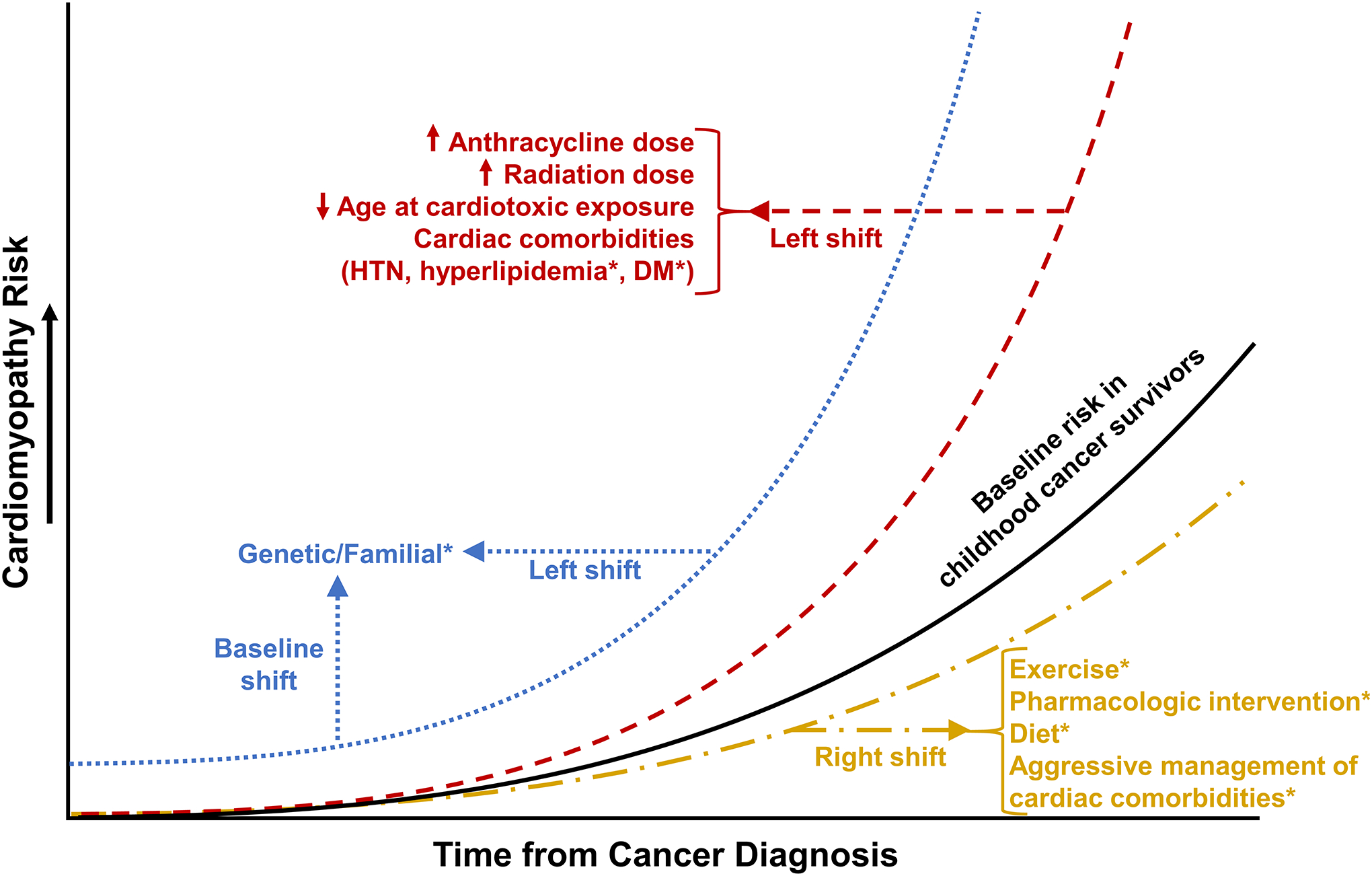
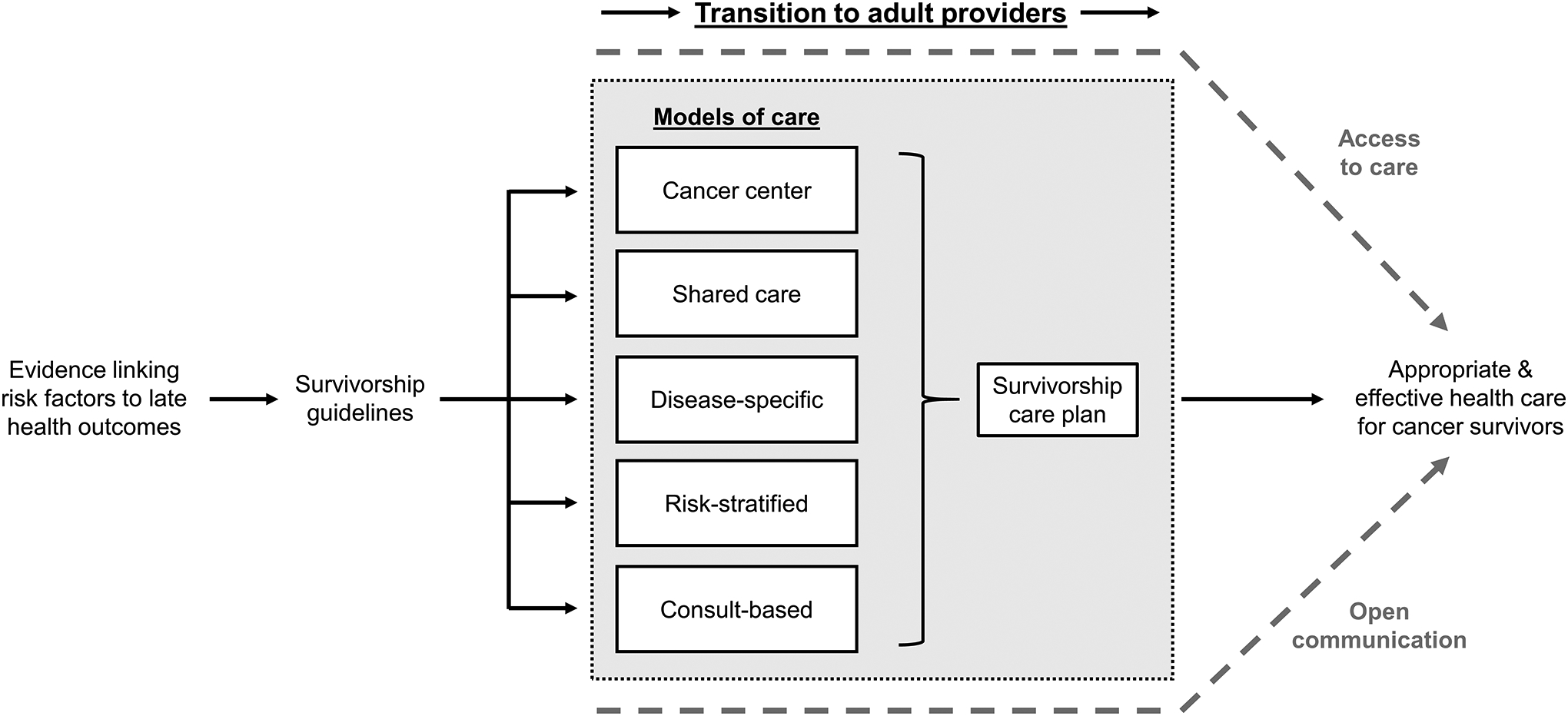
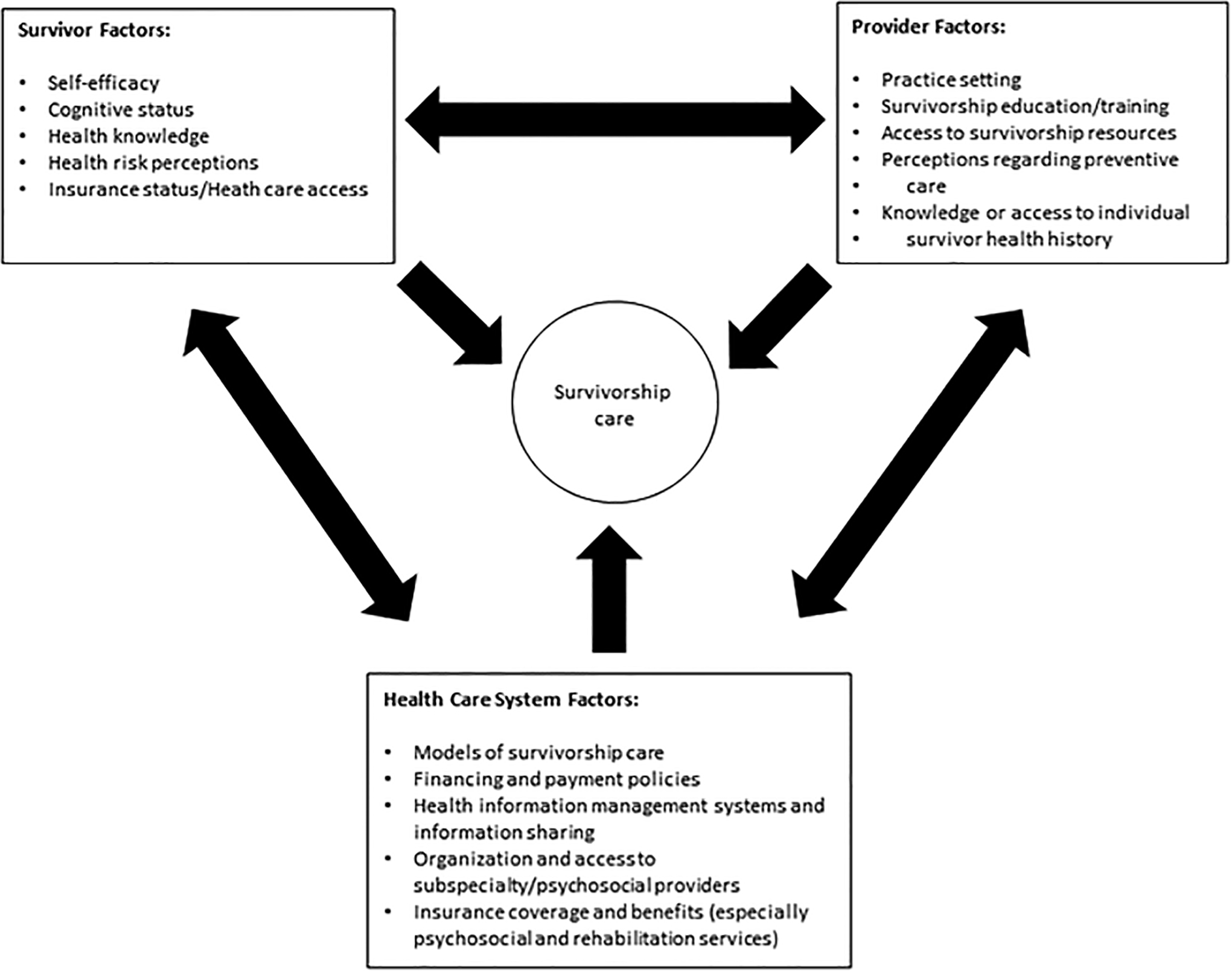
The population of adult survivors of childhood cancer continues to grow as survival rates improve. Although it is well established that these survivors experience various complications and comorbidities related to their malignancy and treatment, this risk is modified by many factors that are not directly linked to their cancer history. Research evaluating the influence of patient-specific demographic and genetic factors, premorbid and comorbid conditions, health behaviors, and aging has identified additional risk factors that influence cancer treatment-related toxicity and possible targets for intervention in this population. Furthermore, although current long-term follow-up guidelines comprehensively address specific therapy-related risks and provide screening recommendations, the risk profile of the population continues to evolve with ongoing modification of treatment strategies and the emergence of novel therapeutics. To address the multifactorial modifiers of cancer treatment-related health risk and evolving treatment approaches, a patient-centered and risk-adapted approach to care that often requires a multidisciplinary team approach, including medical and behavioral providers, is necessary for this population. CA Cancer J Clin 2018;68:133-152. © 2018 American Cancer Society.
Keywords: adolescent; antineoplastic agents; cancer; child; delivery of health care; neoplasms; risk; survivors; treatment outcome.
© 2018 American Cancer Society.
Figures
References
-
- Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2014. Bethesda, MD: National Cancer Institute; 2017.
-
- Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2017. CA Cancer J Clin. 2017;67(1):7–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
