

Diagnostic performance of 18F-FDG PET/CT using point spread function reconstruction on initial staging of rectal cancer: a comparison study with conventional PET/CT and pelvic MRI
- PMID: 29378659
- PMCID: PMC5789619
- DOI: 10.1186/s40644-018-0137-9
Diagnostic performance of 18F-FDG PET/CT using point spread function reconstruction on initial staging of rectal cancer: a comparison study with conventional PET/CT and pelvic MRI
Abstract
Background: Accurate staging is crucial for treatment selection and prognosis prediction in patients with rectal cancer. Point spread function (PSF) reconstruction can improve spatial resolution and signal-to-noise ratio of PET imaging. The aim of this study was to evaluate the effectiveness of 18F-FDG PET/CT with PSF reconstruction for initial staging in rectal cancer compared with conventional PET/CT and pelvic MRI.
Methods: A total of 59 patients with rectal cancer underwent preoperative 18F-FDG PET/CT and pelvic MRI. The maximum standardized uptake value (SUVmax) and lesion to background (L/B) ratio of possible metastatic lymph nodes, and metabolic tumor volumes (MTVs) of primary tumors were calculated. For N and T (T1-2 vs T3-4) staging, sensitivities, specificities, positive predictive values, negative predictive values, and accuracies were compared between conventional PET/CT [reconstructed with ordered subset expectation maximization (OSEM)], PSF-PET/CT (reconstructed with OSEM+PSF), and pelvic MRI. Histopathologic analysis was the reference standard.
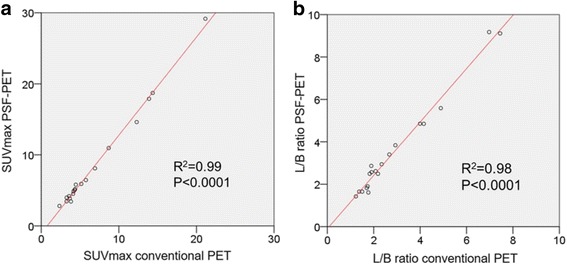
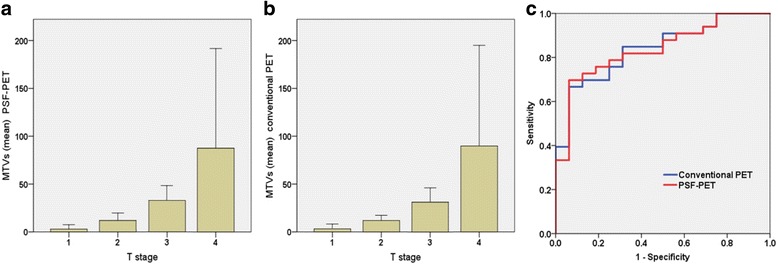
Results: For N staging, PSF-PET/CT provided higher sensitivity (78.6%) than conventional PET/CT (64.3%), and pelvic MRI (57.1%), and all techniques showed high specificity (PSF-PET: 95.4%, conventional PET: 96.7%, pelvic MRI: 93.5%). SUVmax and L/B ratio were significantly higher in PSF-PET/CT than conventional-PET/CT (p < 0.001). The accuracy for T staging in PSF-PET/CT (69.4%) was not significantly different to conventional PET/CT (73.5%) and pelvic MRI (73.5%). MTVs of PSF and conventional PET showed a significant difference among T stages (p < 0.001), with higher values in advanced stages. In M staging, both PSF and conventional PET/CT diagnosed all distant metastases correctly.
Conclusions: PSF-PET/CT produced images with higher lesion-to-background contrast than conventional PET/CT, which allowed improved detection of lymph node metastasis without compromising specificity, and showed comparable diagnostic value to MRI in local staging. PSF-PET/CT is likely to have a great value for initial staging in rectal cancer.
Keywords: 18F-FDG pet/ct; Pelvic MRI; Point spread function (PSF); Rectal cancer; Staging.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent: Informed consent was waived by the Institutional Review Board because of the retrospective nature of the study and the analysis used anonymous clinical data.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
