

A Multicenter, Randomized, Double-Blind, Phase 2 Study of the Efficacy and Safety of Plazomicin Compared with Levofloxacin in the Treatment of Complicated Urinary Tract Infection and Acute Pyelonephritis
- PMID: 29378708
- PMCID: PMC5913993
- DOI: 10.1128/AAC.01989-17
A Multicenter, Randomized, Double-Blind, Phase 2 Study of the Efficacy and Safety of Plazomicin Compared with Levofloxacin in the Treatment of Complicated Urinary Tract Infection and Acute Pyelonephritis
Abstract
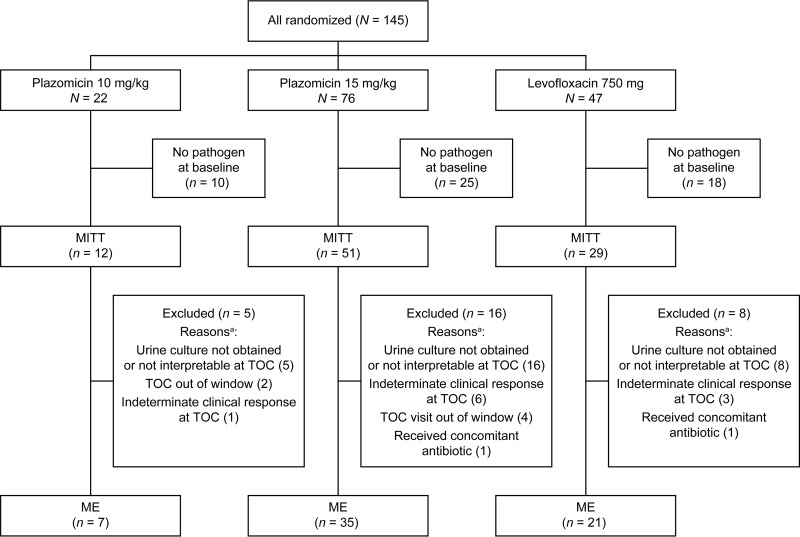
Increasing antimicrobial resistance among uropathogens limits treatment options for patients with complicated urinary tract infection (cUTI). Plazomicin, a new aminoglycoside, has in vitro activity against multidrug-resistant Enterobacteriaceae, including isolates resistant to currently available aminoglycosides, as well as extended-spectrum β-lactamase-producing and carbapenem-resistant Enterobacteriaceae We evaluated the efficacy and safety of plazomicin in a double-blind, comparator-controlled, phase 2 study in adults with cUTI or acute pyelonephritis. Patients were randomized 1:1:1 to receive intravenous plazomicin (10 or 15 mg/kg of body weight) or intravenous levofloxacin (750 mg) once daily for 5 days. Coprimary efficacy endpoints were microbiological eradication at the test of cure (TOC; 5 to 12 days after the last dose) in the modified intent-to-treat (MITT) and microbiologically evaluable (ME) populations. Overall, 145 patients were randomized to treatment. In the groups receiving plazomicin at 10 mg/kg, plazomicin at 15 mg/kg, and levofloxacin, microbiological eradication rates were, respectively, 50.0% (6 patients with microbiological eradication at TOC/12 patients treated [95% confidence interval {CI}, 21.1 to 78.9%]), 60.8% (31/51 [95% CI, 46.1 to 74.2%]), and 58.6% (17/29 [95% CI, 38.9 to 76.5%]) in the MITT population and 85.7% (6/7 [95% CI, 42.1 to 99.6%]), 88.6% (31/35 [95% CI, 73.3 to 96.8%]), and 81.0% (17/21 [95% CI, 58.1 to 94.6%]) in the ME population. In the MITT population, 66.7% (95% CI, 34.9 to 90.1%), 70.6% (95% CI, 56.2 to 82.5%), and 65.5% (95% CI, 45.7 to 82.1%) of the patients in the three groups, respectively, were assessed by the investigator to be clinically cured at TOC. Adverse events were reported in 31.8%, 35.1%, and 47.7% of the patients in the three groups, respectively. Serum creatinine values were generally stable over the course of the study. No plazomicin-treated patients with evaluable audiometry data had postbaseline sensorineural, conductive, or mixed hearing loss. In summary, plazomicin demonstrated microbiological and clinical success and an overall safety profile supportive of further clinical development. (This study has been registered at ClinicalTrials.gov under identifier NCT01096849.).
Keywords: aminoglycosides; antibacterial therapy; clinical trials; complicated urinary tract infection; plazomicin; pyelonephritis.
Copyright © 2018 American Society for Microbiology.
Figures
References
-
- Cek M, Tandogdu Z, Wagenlehner F, Tenke P, Naber K, Bjerklund-Johansen TE. 2014. Healthcare-associated urinary tract infections in hospitalized urological patients—a global perspective: results from the GPIU studies 2003-2010. World J Urol 32:1587–1594. doi: 10.1007/s00345-013-1218-9. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
