

Spinal dysraphism illustrated; Embroyology revisited
- PMID: 29379236
- PMCID: PMC5761168
- DOI: 10.4103/ijri.IJRI_451_16
Spinal dysraphism illustrated; Embroyology revisited
Abstract
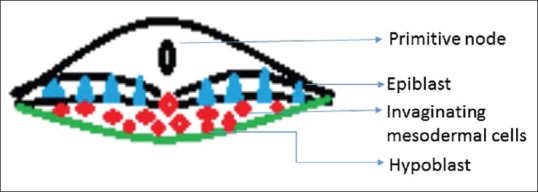
Spinal cord development occurs through three consecutive periods of gastrulation, primary nerulation and secondary neurulation. Aberration in these stages causes abnormalities of the spine and spinal cord, collectively referred as spinal dysraphism. They can be broadly classified as anomalies of gastrulation (disorders of notochord formation and of integration); anomalies of primary neurulation (premature dysjunction and nondysjunction); combined anomalies of gastrulation and primary neurulation and anomalies of secondary neurulation. Correlation with clinical and embryological data and common imaging findings provides an organized approach in their diagnosis.
Keywords: Embryology; illustrated; magnetic resonance imaging; spinal dysraphism.
Conflict of interest statement
There are no conflicts of interest.
Figures




















References
-
- Barkovich AJ, Millen KJ, Dobyns WB. A developmental classification of malformations of the brainstem. Ann Neurol. 2007;62:625–39. - PubMed
-
- Parisi MA, Dobyns WB. Human malformations of the midbrain and hindbrain: Review and proposed classification scheme. Mol Genet Metab. 2003;80:36–53. - PubMed
-
- Tortori-Donati P, Rossi A, Cama A. Spinal dysraphism: A review of neuroradiological features with embryological correlations and proposal for a new classification. Neuroradiology. 2000;42:471–91. - PubMed
-
- Rufener S, Ibrahim M, Parmar HA. Imaging of Congenital Spine and Spinal Cord Malformations. Neuroimaging Clin N Am. 2011;21:659–76. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources