

Endovascular uterine artery interventions
- PMID: 29379246
- PMCID: PMC5761178
- DOI: 10.4103/ijri.IJRI_204_16
Endovascular uterine artery interventions
Abstract
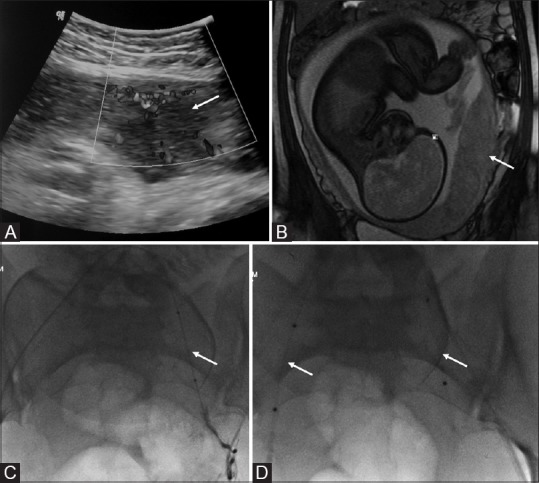
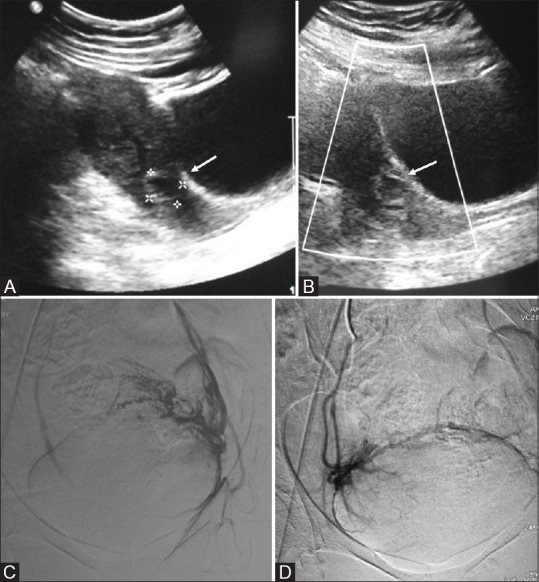
Percutaneous vascular embolization plays an important role in the management of various gynecologic and obstetric abnormalities. Transcatheter embolization is a minimally invasive alternative procedure to surgery with reduced morbidity and mortality, and preserves the patient's future fertility potential. The clinical indications for transcatheter embolization are much broader and include many benign gynecologic conditions, such as fibroid, adenomyosis, and arteriovenous malformations (AVMs), as well as intractable bleeding due to inoperable advanced-stage malignancies. The most well-known and well-studied indication is uterine fibroid embolization. Uterine artery embolization (UAE) may be performed to prevent or treat bleeding associated with various obstetric conditions, including postpartum hemorrhage (PPH), placental implantation abnormality, and ectopic pregnancy. Embolization of the uterine artery or the internal iliac artery also may be performed to control pelvic bleeding due to coagulopathy or iatrogenic injury. This article discusses these gynecologic and obstetric indications for transcatheter embolization and reviews procedural techniques and outcomes.
Keywords: Angiography; embolization; uterine artery.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Andrews RT, Spies JB, Sacks D, Worthington-Kirsch RL, Niedzwiecki GA, Marx MV, et al. Patient care and uterine artery embolization for leiomyomata. J Vasc Interv Radiol. 2009;20:S307–11. - PubMed
-
- Bulman JC, Ascher SM, Spies JB. Current concepts in uterine fibroid embolization. Radiographics. 2012;32:1735–50. - PubMed
-
- Resnick NJ, Kim E, Patel RS, Lookstein RA, Nowakowski FS, Fischman AM. Uterine artery embolization using a transradial approach: Initial experience and technique. J Vasc Interv Radiol. 2014;25:443–7. - PubMed
-
- Pelage JP, Le Dref O, Soyer P, Jacob D, Kardache M, Dahan H, et al. Arterial anatomy of the female genital tract: Variations and relevance to transcatheter embolization of the uterus. AJR Am J Roentgenol. 1999;172:989–94. - PubMed
-
- Binkert CA, Hirzel FC, Gutzeit A, Zollikofer CL, Hess T. Superior hypogastric nerve block to reduce pain after uterine artery embolization: Advanced technique and comparison to epidural anesthesia. Cardiovasc Intervent Radiol. 2015;38:1157–61. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources