

Anal and Perineal Injuries
- PMID: 29379404
- PMCID: PMC5787399
- DOI: 10.1055/s-0037-1602176
Anal and Perineal Injuries
Abstract
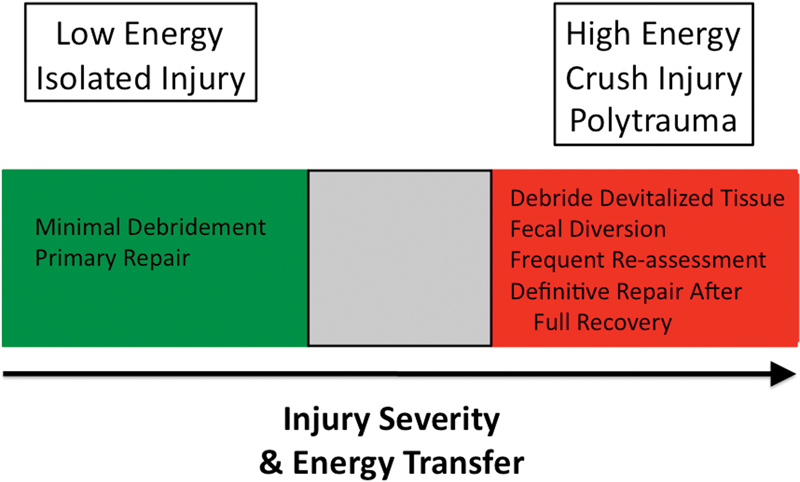
With increased use of explosive devices in warfare, anal trauma is often seen coupled with more complex pelviperineal injury. While the associated mortality is high, casualties that survive are often left with disabling fecal incontinence from damage to the anosphincteric complex. After resolution of the acute insult, the initial evaluation mandates a thorough physical exam, including endoscopic evaluation with rigid proctoscopy and flexible sigmoidoscopy, as well as adjunctive testing, specifically anal manometry and endoanal ultrasound. First-line therapy favors bulking agents and antidiarrheals, in conjunction with biofeedback, due to a minimal risk profile. Surgical options range from direct sphincter repairs to complex anosphincteric reconstruction with widely variable results. Most recently, burgeoning therapies in the treatment of fecal incontinence, including sacral nerve stimulation and magnetic anal sphincters, offer excellent alternatives with promising long-term outcomes. In summation, the goal of all interventions is the re-establishment of bowel continence, but, in its absence, permanent fecal diversion for devastating fecal incontinence is a reasonable option with excellent patient satisfaction scores.
Keywords: anal and perineal trauma; anosphincteric complex; fecal incontinence.
Conflict of interest statement
Figures

References
-
- Kudsk K A, Hanna M K. Management of complex perineal injuries. World J Surg. 2003;27(08):895–900. - PubMed
-
- Mossadegh S, Tai N, Midwinter M, Parker P. Improvised explosive device related pelvi-perineal trauma: anatomic injuries and surgical management. J Trauma Acute Care Surg. 2012;73(02) 01:S24–S31. - PubMed
-
- Tai N R, Russell R. Right turn resuscitation: frequently asked questions. J R Army Med Corps. 2011;157(03) 01:S310–S314. - PubMed
-
- Glasgow S C, Heafner T A, Watson J DB, Aden J K, Perry W B. Initial management and outcome of modern battlefield anal trauma. Dis Colon Rectum. 2014;57(08):1012–1018. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
