

Decline in Prescription Opioids Attributable to Decreases in Long-Term Use: A Retrospective Study in the Veterans Health Administration 2010-2016
- PMID: 29380212
- PMCID: PMC5975137
- DOI: 10.1007/s11606-017-4283-8
Decline in Prescription Opioids Attributable to Decreases in Long-Term Use: A Retrospective Study in the Veterans Health Administration 2010-2016
Abstract
Background: Improved understanding of temporal trends in short- and long-term opioid prescribing may inform efforts to curb the opioid epidemic.
Objective: To characterize the prevalence of short- and long-term opioid prescribing in the Veterans Health Administration (VHA) from 2010 to 2016.
Design: Observational cohort study using VHA databases.
Participants: All patients receiving at least one outpatient prescription through the VHA during calendar years 2010 through 2016.
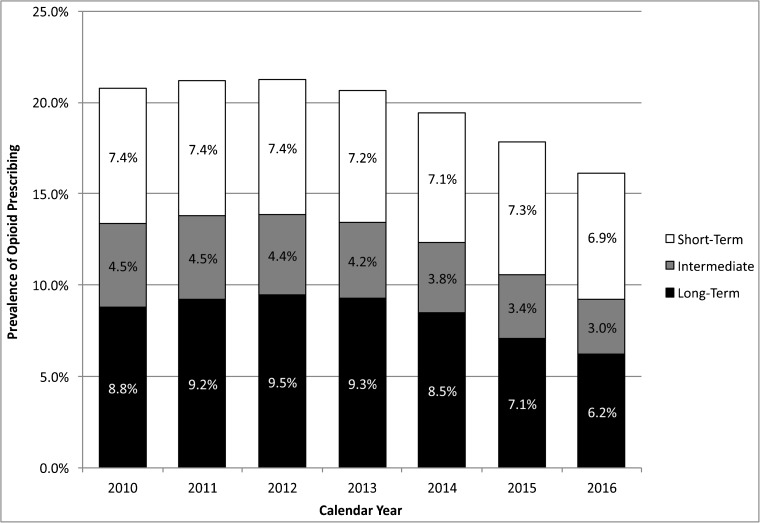
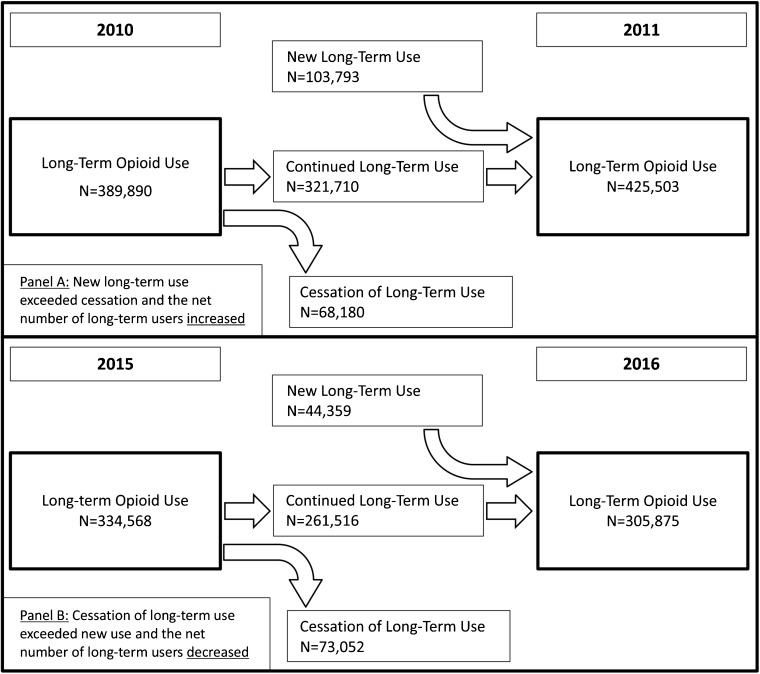
Main measures: Prevalence of opioid use from 2010 through 2016, stratified by short-term, intermediate-term, and long-term use. Temporal trends in discontinuation among existing long-term users and initiation of new long-term use and the net impact on rates of long-term opioid use. Relative likelihood of transitioning to long-term opioid use contrasted with use patterns in the prior year.
Key results: The prevalence of opioid prescribing was 20.8% in 2010, peaked at 21.2% in 2012, and declined annually to 16.1% in 2016. Between 2010 and 2016, reductions in long-term opioid prescribing accounted for 83% of the overall decline in opioid prescription fills. Comparing data from 2010-2011 to data from 2015-2016, declining rates in new long-term use accounted for more than 90% of the decreasing prevalence of long-term opioid use in the VHA, whereas increases in cessation among existing long-term users accounted for less than 10%. The relative risk of transitioning to long-term use during 2016 was 6.5 (95% CI: 6.4, 6.7) among short-term users and 35.5 (95% CI: 34.8, 36.3) among intermediate users, relative to patients with no opioid prescriptions filled during 2015.
Conclusions: Opioid prescribing trends followed similar trajectories in VHA and non-VHA settings, peaking around 2012 and subsequently declining. However, changes in long-term opioid prescribing accounted for most of the decline in the VHA. Recent VA opioid initiatives may be preventing patients from initiating long-term use. This may offer valuable lessons generalizable to other healthcare systems.
Keywords: opioid; prevalence; veteran.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Comment in
-
Reducing Long-term Opioid Use in the Veterans Health Administration.J Gen Intern Med. 2018 Jun;33(6):781-782. doi: 10.1007/s11606-018-4352-7. J Gen Intern Med. 2018. PMID: 29450685 Free PMC article. No abstract available.
References
-
- Prescription Drug Monitoring Program Training and Technical Assistance Center. Available at: http://www.pdmpassist.org. Accessed December 12, 2017.
-
- Drug Enforcement Administration, Department of Justice. Schedules of controlled substances: rescheduling of hydrocodone combination products from schedule III to schedule II. Final rule. Fed Regist. 2014;79(163):49661–82. - PubMed
-
- Huff, C. States aim to limit opioid prescriptions. ACP Internist. 2016. Available at: https://acpinternist.org/archives/2016/10/laws.htm. Accessed December 12, 2017.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
