

Comparison of outcomes in hematological malignancies treated with haploidentical or HLA-identical sibling hematopoietic stem cell transplantation following myeloablative conditioning: A meta-analysis
- PMID: 29381772
- PMCID: PMC5790250
- DOI: 10.1371/journal.pone.0191955
Comparison of outcomes in hematological malignancies treated with haploidentical or HLA-identical sibling hematopoietic stem cell transplantation following myeloablative conditioning: A meta-analysis
Abstract
Purpose: Haploidentical and human leukocyte antigen (HLA)-identical sibling hematopoietic stem transplantation are two main ways used in allogeneic hematopoietic stem cell transplantation (allo-HSCT). In recent years, remarkable progress has been made in haploidentical allo-HSCT (HID-SCT), and some institutions found HID-SCT had similar outcomes as HLA-identical sibling allo-HSCT (ISD-SCT). To clarify if HID-SCT has equal effects to ISD-SCT in hematologic malignancies, we performed this meta-analysis.
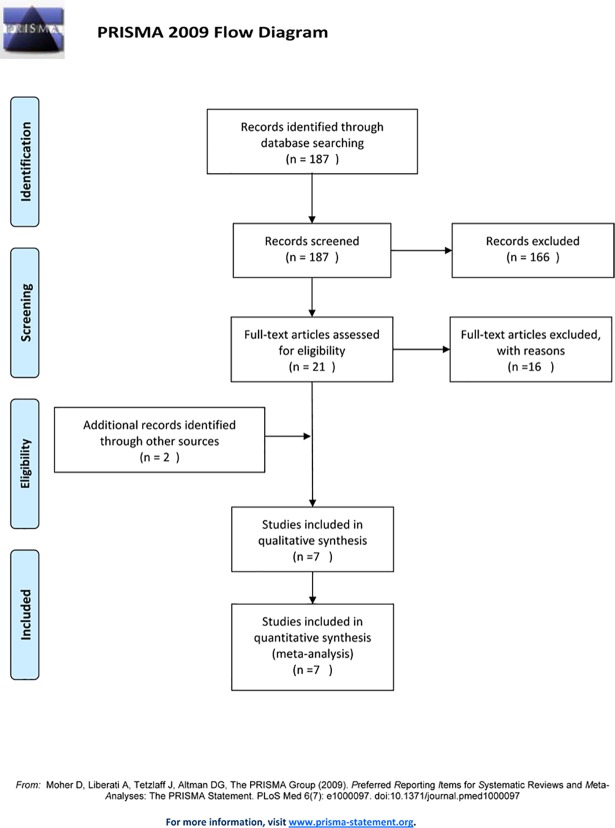
Methods: Relevant articles published prior to February 2017 were searched on PubMed. Two reviewers assessed the quality of the included studies and extracted data independently. Odds ratio (OR) and 95% confidence intervals (CIs) were calculated for statistical analysis.
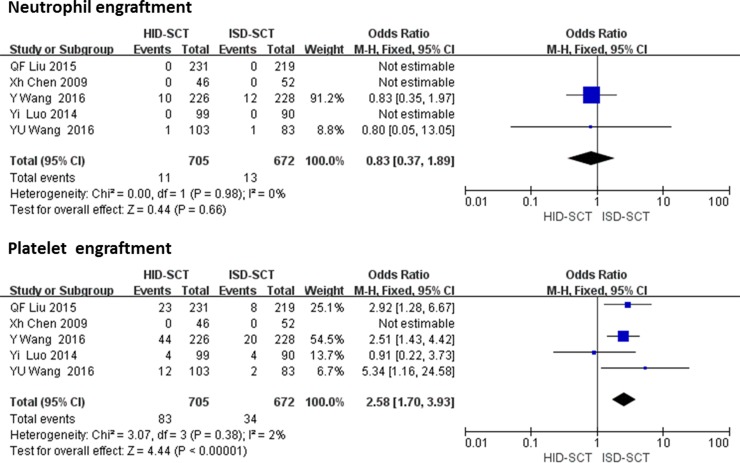
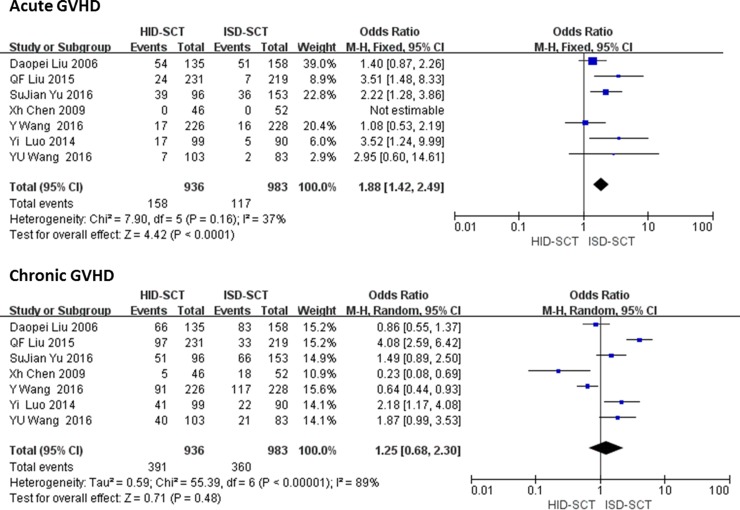
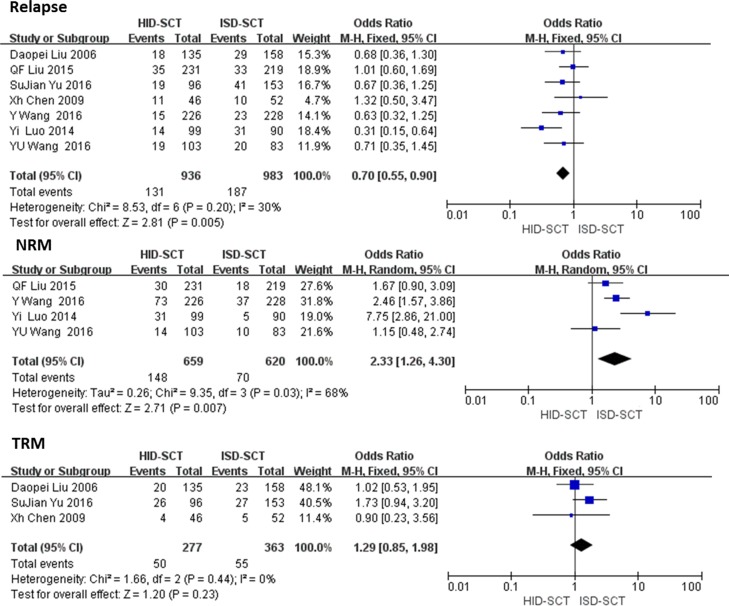
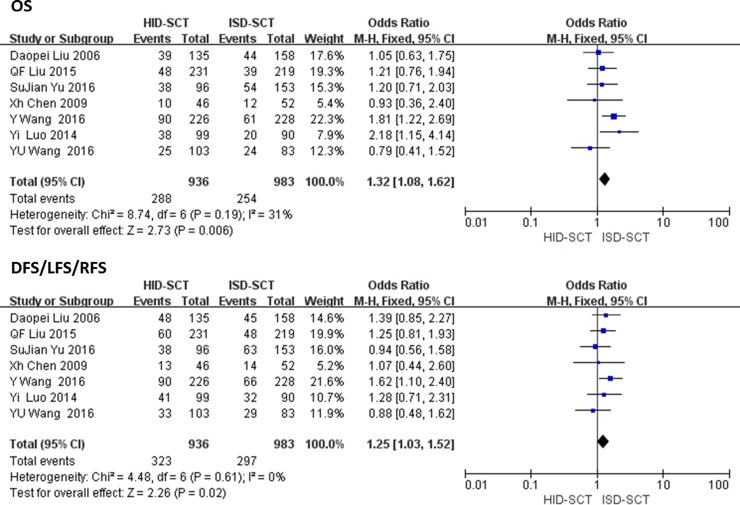
Results: Seven studies including 1919 patients were included. The rate of platelet engraftment is significantly lower after HID-SCT versus ISD-SCT while there is no difference in neutrophil engraftment (OR = 2.58, 95% CI = 1.70-3.93, P < 0.00001). The risk of acute graft-versus-host disease (GVHD) is significantly higher after HID-SCT versus ISD-SCT (OR = 1.88, 95% CI = 1.42-2.49, P < 0.00001), but the relapse rate is lower in HID-SCT group (OR = 0.70, 95% CI = 0.55-0.90, P = 0.005). The incidence rates of overall survival (OS) and disease-free-survival/leukemia-free survival/relapse-free survival (DFS/LFS/RFS) after ISD-SCT are all significantly superior to HID-SCT (OR = 1.32, 95% CI = 1.08-1.62, P = 0.006; OR = 1.25, 95% CI = 1.03-1.52, P = 0.02). There is no significant difference in transplantation related mortality (TRM) rate after HID-SCT and ISD-SCT.
Conclusion: After myeloablative conditioning, patients receiving ISD-SCT have a faster engraftment, lower acute GVHD and longer life expectancy compared to HID-SCT with GVHD prophylaxis (cyclosporine A, methotrexate, mycophenolate mofetil and antithymoglobulin; CsA + MTX + MMF + ATG). Currently, HID-SCT with GVHD prophylaxis (CsA + MTX + MMF + ATG) may not replace ISD-SCT when HLA-identical sibling donor available.
Conflict of interest statement
Figures
Similar articles
-
Superior graft-versus-leukemia effect associated with transplantation of haploidentical compared with HLA-identical sibling donor grafts for high-risk acute leukemia: an historic comparison.Biol Blood Marrow Transplant. 2011 Jun;17(6):821-30. doi: 10.1016/j.bbmt.2010.08.023. Epub 2010 Sep 8. Biol Blood Marrow Transplant. 2011. PMID: 20831895
-
Haploidentical- versus identical-sibling transplant for high-risk pediatric AML: A multi-center study.Cancer Commun (Lond). 2020 Mar;40(2-3):93-104. doi: 10.1002/cac2.12014. Epub 2020 Mar 16. Cancer Commun (Lond). 2020. PMID: 32175698 Free PMC article.
-
Patients receiving HLA-haploidentical/partially matched related allo-HSCT can achieve desirable health-related QoL that is comparable to that of patients receiving HLA-identical sibling allo-HSCT.Bone Marrow Transplant. 2012 Sep;47(9):1201-5. doi: 10.1038/bmt.2011.250. Epub 2012 Jan 9. Bone Marrow Transplant. 2012. PMID: 22231459
-
Efficacy and safety of mesenchymal stem cells co-infusion in allogeneic hematopoietic stem cell transplantation: a systematic review and meta-analysis.Stem Cell Res Ther. 2021 Apr 20;12(1):246. doi: 10.1186/s13287-021-02304-x. Stem Cell Res Ther. 2021. PMID: 33879242 Free PMC article.
-
Haploidentical stem cell transplantation vs matched unrelated donor transplantation in adults with hematologic malignancies: a systematic review and meta-analysis.Hematology. 2020 Dec;25(1):356-365. doi: 10.1080/16078454.2020.1831292. Hematology. 2020. PMID: 33054609
Cited by
-
Myeloablative Haploidentical Transplant as an Alternative to Matched Sibling Transplant for Peripheral T-Cell Lymphomas.Cell Transplant. 2021 Jan-Dec;30:963689721999615. doi: 10.1177/0963689721999615. Cell Transplant. 2021. PMID: 33745341 Free PMC article.
-
Late Complications of Allogenic Stem Cells Transplantation in Leukaemia.Tissue Eng Regen Med. 2018 Sep 6;16(1):1-9. doi: 10.1007/s13770-018-0157-3. eCollection 2019 Feb. Tissue Eng Regen Med. 2018. PMID: 30815345 Free PMC article. Review.
-
Haploidentical Stem Cell Transplantation With Posttransplant Cyclophosphamide Therapy vs Other Donor Transplantations in Adults With Hematologic Cancers: A Systematic Review and Meta-analysis.JAMA Oncol. 2019 Dec 1;5(12):1739-1748. doi: 10.1001/jamaoncol.2019.3541. JAMA Oncol. 2019. PMID: 31621796 Free PMC article.
-
Granulocyte Colony-Stimulating Factor-Primed Unmanipulated Haploidentical Blood and Marrow Transplantation.Front Immunol. 2019 Nov 1;10:2516. doi: 10.3389/fimmu.2019.02516. eCollection 2019. Front Immunol. 2019. PMID: 31749802 Free PMC article. Review.
-
A Prospective Trial Comparing Haploidentical Donor Transplantation With Cord Blood Versus HLA-Matched Sibling Donor Transplantation for Hematologic Malignancy Patients.Cell Transplant. 2022 Jan-Dec;31:9636897221076050. doi: 10.1177/09636897221076050. Cell Transplant. 2022. PMID: 35168385 Free PMC article.
References
-
- Ballen K, Gluckman E, Broxmeyer HE. Umbilical cord blood transplantation: the first 25 years and beyond. Blood.2013; 122(4):491–498. doi: 10.1182/blood-2013-02-453175 - DOI - PMC - PubMed
-
- Luznik L, O’Donnell PV, Symons HJ, Chen AR, Leffell MS, Zahurak M, et al. HLA haploidentical bone marrow transplantation for hematologic malignancies using nonmyeloablative conditioning and high-dose, posttransplantation cyclophosphamide. Biol Blood Marrow Transplant. 2008; 14(6): 641–650. doi: 10.1016/j.bbmt.2008.03.005 - DOI - PMC - PubMed
-
- Di BP, Santarone S, De AG, Picardi A, Cudillo L, Cerretti R, et al. Haploidentical, unmanipulated, G-CSF-primed bone marrow transplantation for patients with high-risk hematologic malignancies. Blood. 2013; 121(5):849–857. doi: 10.1182/blood-2012-08-453399 - DOI - PubMed
-
- Lai Y, Ma J, Schwarzenberger P, Li W, Cai Z, Zhou J, et al. Combination of CsA, MTX and Low–dose, short-course mycophenolate mofetil for GVHD prophylaxis. Bone Marrow Transplant.2009; 43(1):61–67. doi: 10.1038/bmt.2008.265 - DOI - PubMed
-
- Duggan P, Booth K, Chaudhry A, Stewart D, Ruether JD, Glück S, et al. Unrelated donor BMT recipients given pretransplant lowdose antithymocyte globulin have outcomes equivalent to matched sibling BMT: a matched pair analysis. Bone Marrow Transplant.2002; 30(10):681–686. doi: 10.1038/sj.bmt.1703674 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
