

Efficacy and safety of 9 nonoperative regimens for the treatment of spinal cord injury: A network meta-analysis
- PMID: 29381946
- PMCID: PMC5708945
- DOI: 10.1097/MD.0000000000008679
Efficacy and safety of 9 nonoperative regimens for the treatment of spinal cord injury: A network meta-analysis
Abstract
Objective: This network meta-analysis aims to compare the efficacy and safety of 9 nonoperative regimens (placebo, pregabalin, GM-1 ganglioside, venlafaxine extended-release [venlafaxine XR], fampridine, conventional over-ground training [OT], body-weight-supported treadmill training [BWSTT], robotic-assisted gait training [RAGT] + OT and body-weight-supported over-ground training [BWSOT]) in treating spinal cord injury (SCI).
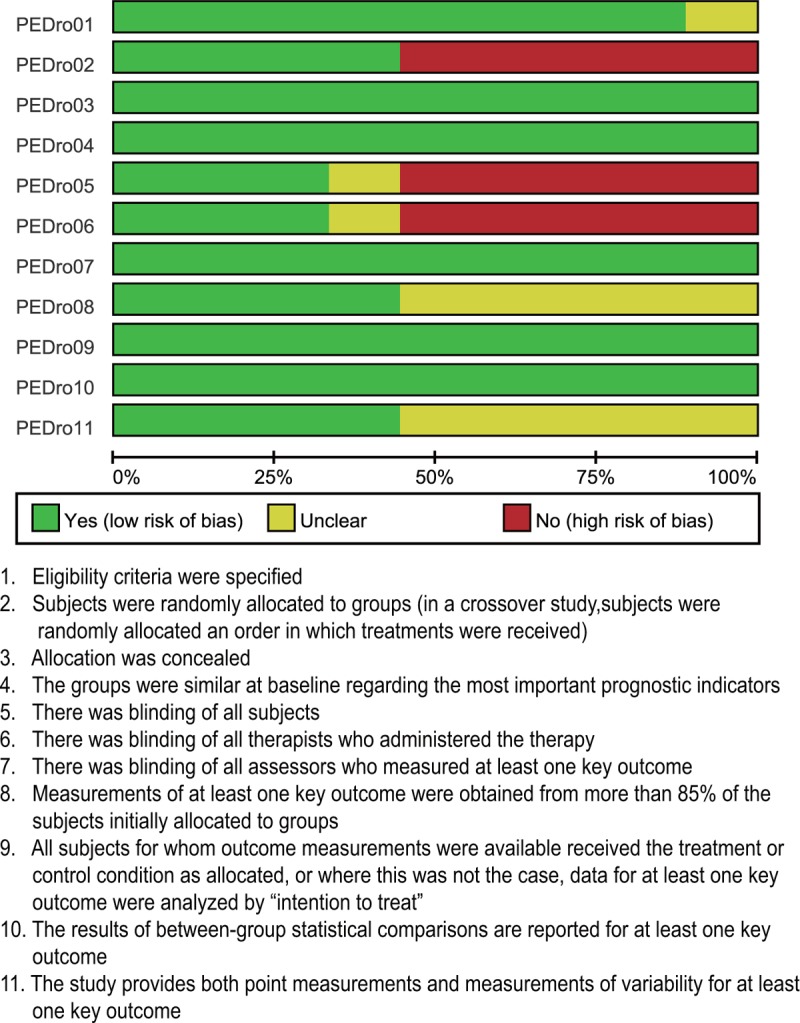
Methods: Clinical controlled trials of 9 nonoperative regimens for SCI were retrieved in the electronic database. Traditional pairwise and Bayesian network meta-analyses were performed to compare the efficacy and safety of 9 nonoperative regimens for the treatment of SCI. Weighted mean difference (WMD), odds ratios (OR), and surface under the cumulative ranking curve (SUCRA) were calculated using the Markov Chain Monte Carlo engine Open BUGS (V.3.4.0) and R (V.3.2.1) package gemtc (V.0.6).
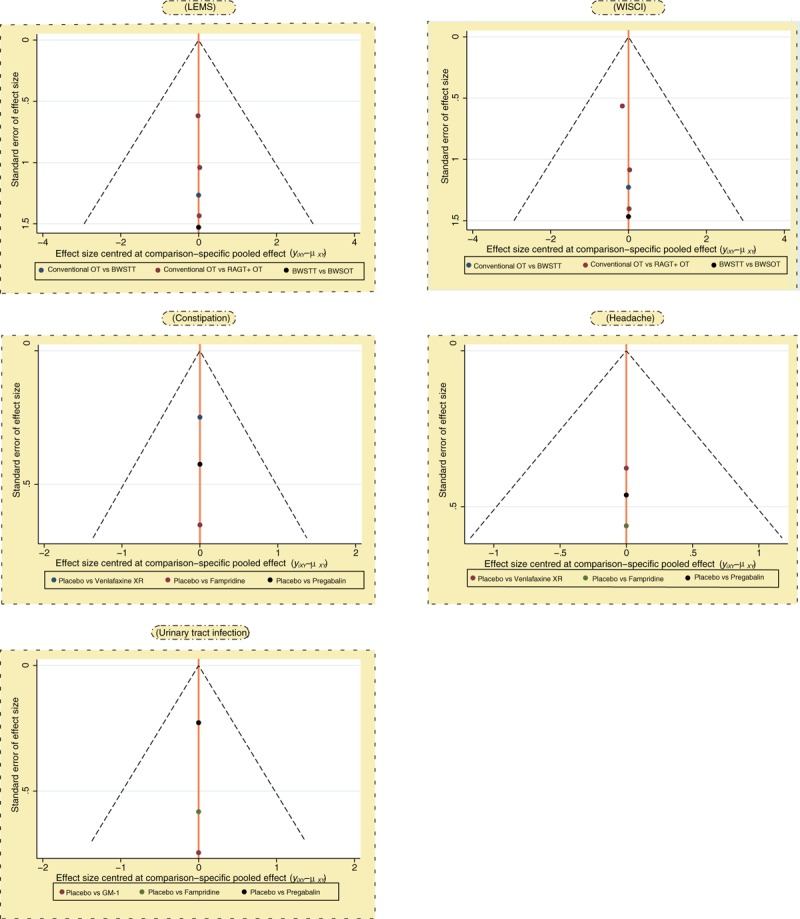
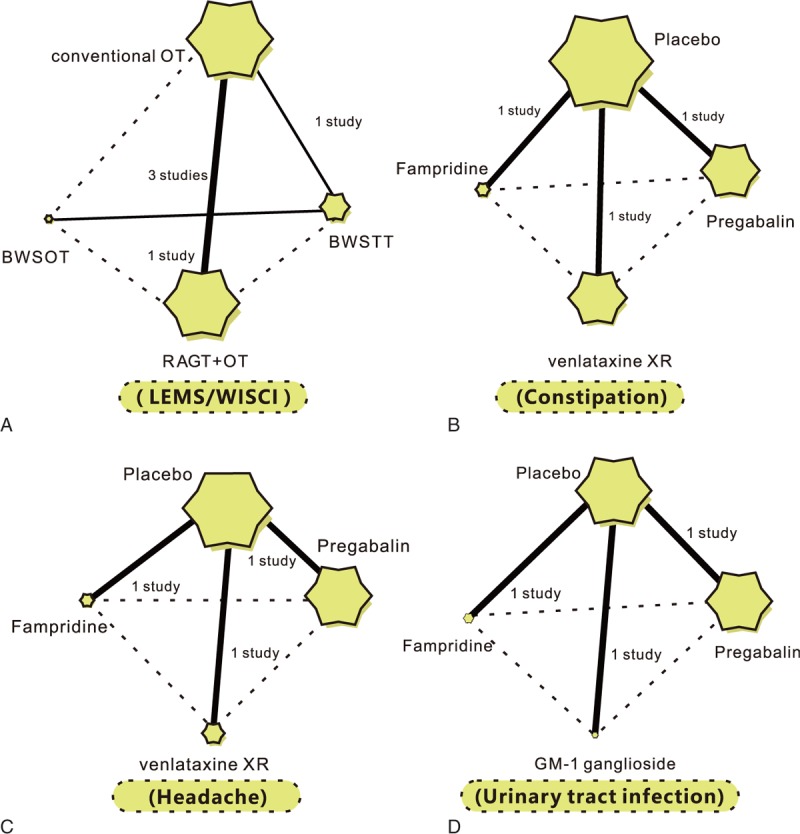
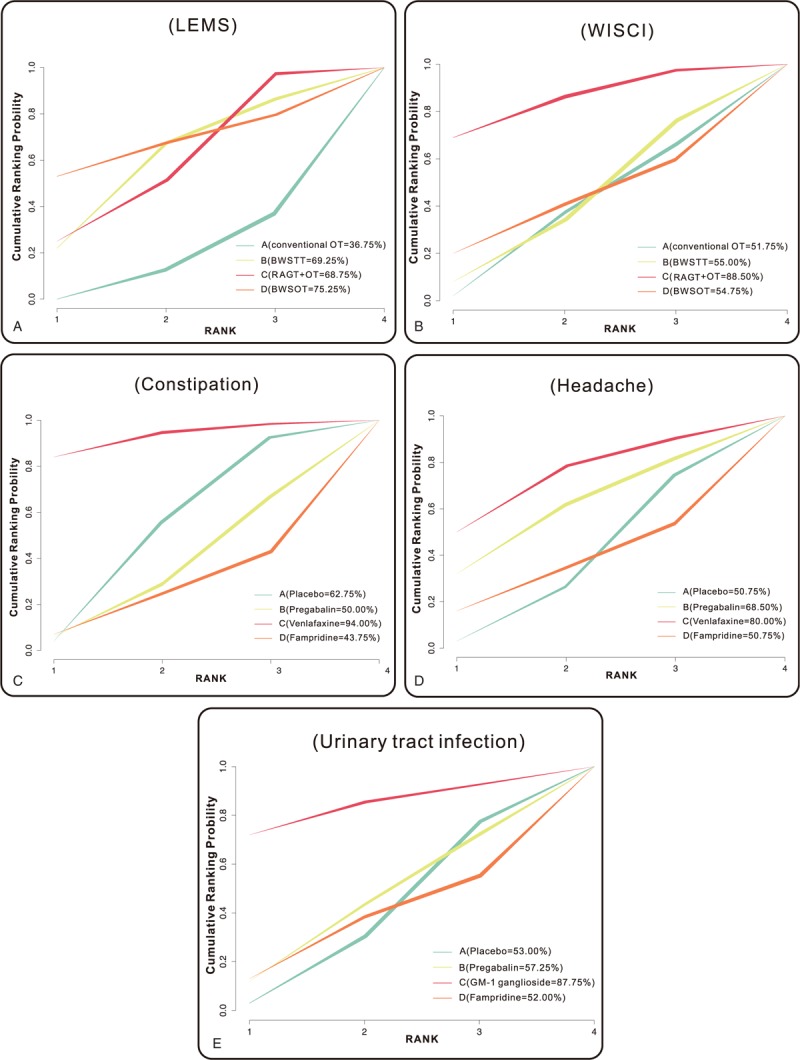
Results: A total of 9 clinical controlled trials meeting the inclusion criteria were selected in this meta-analysis. On the aspect of efficacy, the results of pairwise meta-analysis indicated that the RAGT + OT and BWSOT might have the best efficacy in SCI patients in terms of a lower extremity motor score (LEMS) compared with conventional OT; the efficacy of RAGT + OT on SCI patients was relatively better than that of conventional OT in terms of walking index for spinal cord injury (WISCI). With the aspect of safety, the constipation rate of placebo on SCI patients was relatively higher than that of venlafaxine XR; however, with respect to headache and urinary tract infection, there was no significant difference in the safety of placebo, pregabalin, GM-1 ganglioside, venlafaxine XR, and fampridine on SCI patients. The results of SUCRA values suggested that BWSOT had the highest SUCRA value (75.25%) of LEMS; RAGT + OT had the highest SUCRA value (88.50%) of WISCI; venlafaxine XR had the highest SUCRA value (94.00%) of constipation; venlafaxine XR had the highest SUCRA value (80.00%) of headache; GM-1 ganglioside had the highest SUCRA value (87.75%) of urinary tract infection.
Conclusion: Our results provide evidence that the RAGT + OT and BWSOT might have the best efficacy in the treatment of SCI, and the venlafaxine XR and GM-1 ganglioside showed adequate safety for SCI.
Copyright © 2017 The Authors. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Effects of robotic-assisted gait training on motor function and walking ability in children with thoracolumbar incomplete spinal cord injury.NeuroRehabilitation. 2022;51(3):499-508. doi: 10.3233/NRE-220124. NeuroRehabilitation. 2022. PMID: 35964210 Clinical Trial.
-
Against the odds: what to expect in rehabilitation of chronic spinal cord injury with a neurologically controlled Hybrid Assistive Limb exoskeleton. A subgroup analysis of 55 patients according to age and lesion level.Neurosurg Focus. 2017 May;42(5):E15. doi: 10.3171/2017.2.FOCUS171. Neurosurg Focus. 2017. PMID: 28463613
-
Effects of end-effector robot-assisted gait training on gait ability, muscle strength, and balance in patients with spinal cord injury.NeuroRehabilitation. 2023;53(3):335-346. doi: 10.3233/NRE-230085. NeuroRehabilitation. 2023. PMID: 37638457 Clinical Trial.
-
Which gait training intervention can most effectively improve gait ability in patients with cerebral palsy? A systematic review and network meta-analysis.Front Neurol. 2023 Jan 10;13:1005485. doi: 10.3389/fneur.2022.1005485. eCollection 2022. Front Neurol. 2023. PMID: 36703638 Free PMC article.
-
Effects of robot-assisted gait training on cardiopulmonary function and lower extremity strength in individuals with spinal cord injury: A systematic review and meta-analysis.J Spinal Cord Med. 2024 Jan;47(1):6-14. doi: 10.1080/10790268.2023.2188392. Epub 2023 Mar 27. J Spinal Cord Med. 2024. PMID: 36972206 Free PMC article.
Cited by
-
Acute spinal cord injury: Pathophysiology and pharmacological intervention (Review).Mol Med Rep. 2021 Jun;23(6):417. doi: 10.3892/mmr.2021.12056. Epub 2021 Apr 13. Mol Med Rep. 2021. PMID: 33846780 Free PMC article. Review.
-
Impact of Robotic-Assisted Gait Therapy on Depression and Anxiety Symptoms in Patients with Subacute Spinal Cord Injuries (SCIs)-A Prospective Clinical Study.J Clin Med. 2023 Nov 17;12(22):7153. doi: 10.3390/jcm12227153. J Clin Med. 2023. PMID: 38002765 Free PMC article.
-
Treatment effects of monosialotetrahexosylganglioside on severe traumatic brain injury in adults.Am J Transl Res. 2022 Sep 15;14(9):6638-6646. eCollection 2022. Am J Transl Res. 2022. PMID: 36247290 Free PMC article.
-
The efficacy of gait rehabilitations for the treatment of incomplete spinal cord injury: a systematic review and network meta-analysis.J Orthop Surg Res. 2023 Jan 23;18(1):60. doi: 10.1186/s13018-022-03459-w. J Orthop Surg Res. 2023. PMID: 36683024 Free PMC article.
References
-
- Finnerup NB, Baastrup C. Spinal cord injury pain: mechanisms and management. Curr Pain Headache Rep 2012;16:207–16. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
