

Treatment of aggressive prolactinoma with temozolomide: A case report and review of literature up to date
- PMID: 29381964
- PMCID: PMC5708963
- DOI: 10.1097/MD.0000000000008733
Treatment of aggressive prolactinoma with temozolomide: A case report and review of literature up to date
Abstract
Rationale: Aggressive pituitary adenomas and pituitary carcinomas are rare and demand multiple treatment strategies. Temozolomide, an orally active alkylating chemotherapeutic agent, has recently been recommended as a salvage medication for refractory pituitary adenomas or carcinomas.
Patient concerns: A 17-year-old male presenting with aggressive prolactinoma that continued to progress despite surgery, gamma knife, and dopamine agonists.
Diagnoses: The diagnosis of refractory aggressive prolactinoma was made on the basis of clinical findings and the lack of efficacy of conventional treatment.
Interventions: The patient received the most frequently recommended regimen of temozolomide treatment for 22 cycles.
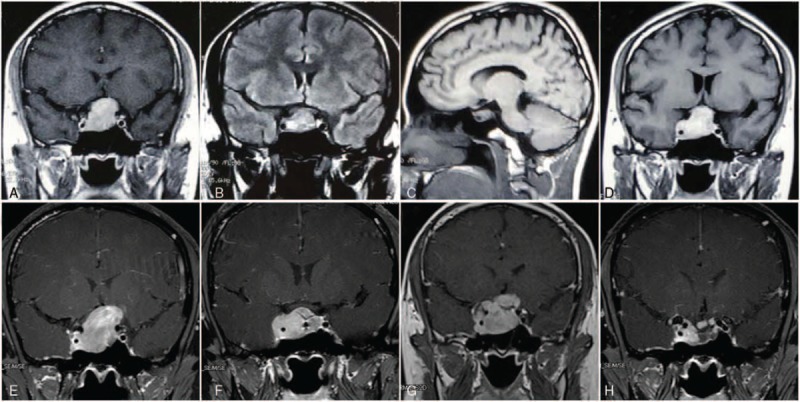
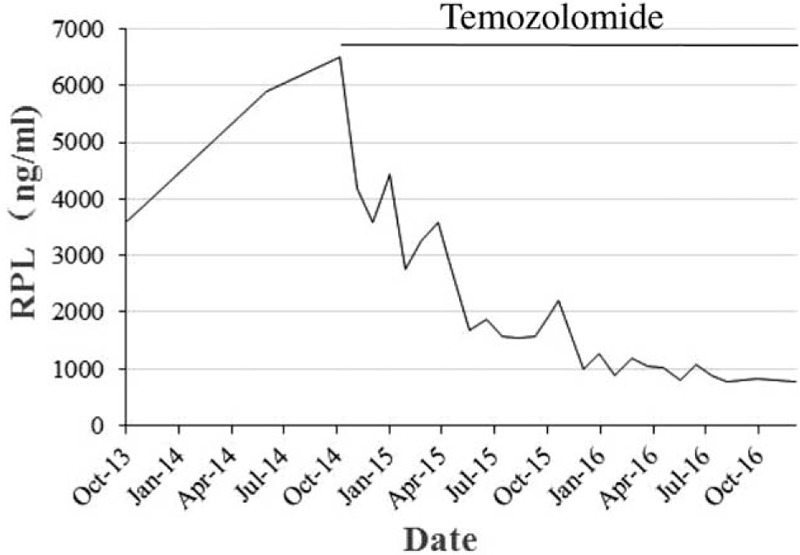
Outcomes: Temozolomide resulted in a remarkable shrinkage of tumor mass and inhibition of prolactin secretion and this patient's clinical condition improved progressively.
Lessons: Temozolomide can be used as a salvage treatment to refractory pituitary tumors and o(6)-methylguanine-DNA methyltransferase (MGMT) status is a significant predictor to the effectiveness of temozolomide based on the existing literature.
Copyright © 2017 The Authors. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Daly AF, Tichomirowa MA, Beckers A. The epidemiology and genetics of pituitary adenomas. Best Pract Res Clin Endocrinol Metab 2009;23:543–54. - PubMed
-
- Molitch ME. Diagnosis and treatment of pituitary adenomas: a review. JAMA 2017;317:516–24. - PubMed
-
- Di Ieva A, Rotondo F, Syro LV, et al. Aggressive pituitary adenomas: diagnosis and emerging treatments. Nat Rev Endocrinol 2014;10:423–35. - PubMed
-
- Chatzellis E, Alexandraki KI, Androulakis II, et al. Aggressive pituitary tumors. Neuroendocrinology 2015;101:87–104. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
