

Preoperative intravenous glucocorticoids can decrease acute pain and postoperative nausea and vomiting after total hip arthroplasty: A PRISMA-compliant meta-analysis
- PMID: 29381983
- PMCID: PMC5708982
- DOI: 10.1097/MD.0000000000008804
Preoperative intravenous glucocorticoids can decrease acute pain and postoperative nausea and vomiting after total hip arthroplasty: A PRISMA-compliant meta-analysis
Erratum in
-
Preoperative intravenous glucocorticoids can decrease acute pain and postoperative nausea and vomiting after total hip arthroplasty: A PRISMA-compliant meta-analysis: Erratum.Medicine (Baltimore). 2018 Jan;97(4):e9728. doi: 10.1097/MD.0000000000009728. Medicine (Baltimore). 2018. PMID: 29369211 Free PMC article. No abstract available.
Abstract
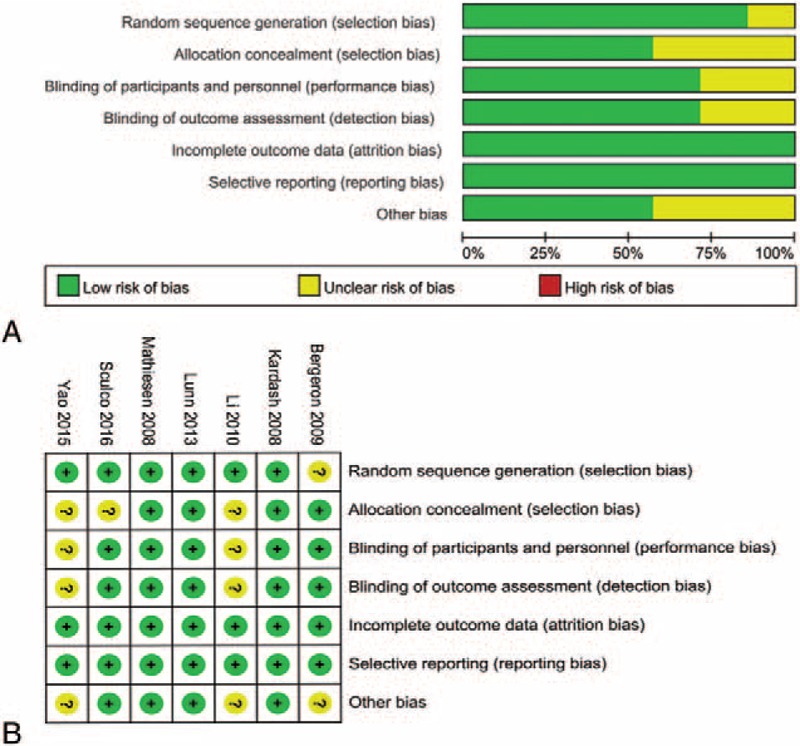
Background: A systematic review and meta-analysis of published randomized controlled trials (RCTs) were performed to assess the efficacy and safety of preoperative intravenous glucocorticoids versus controls for the prevention of postoperative acute pain and postoperative nausea and vomiting (PONV) after primary total hip arthroplasty (THA).
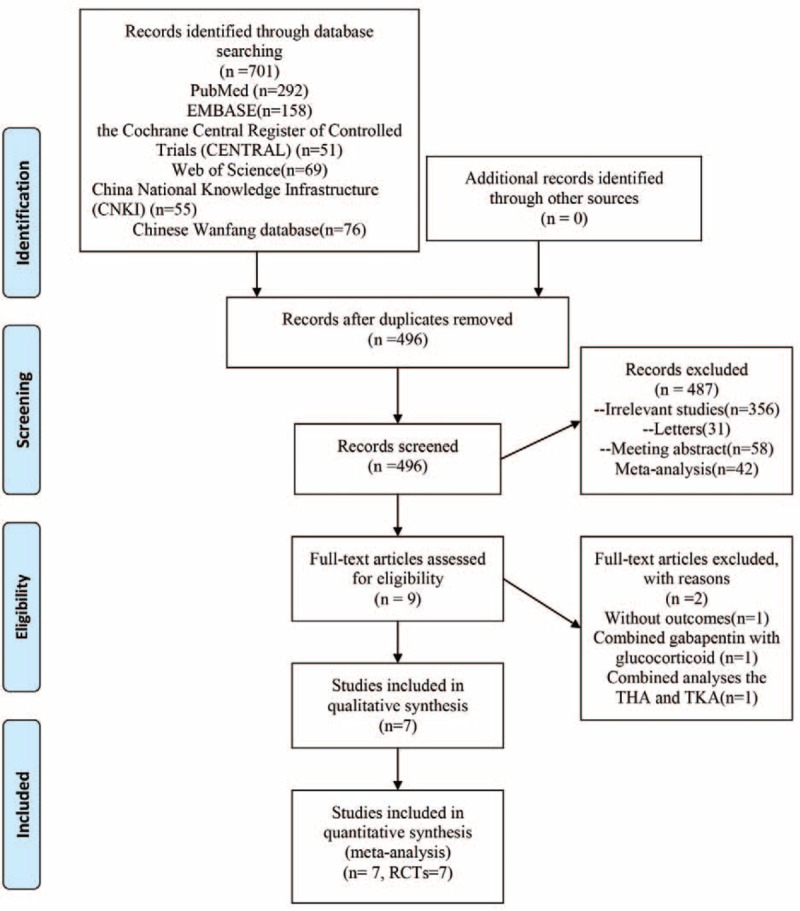
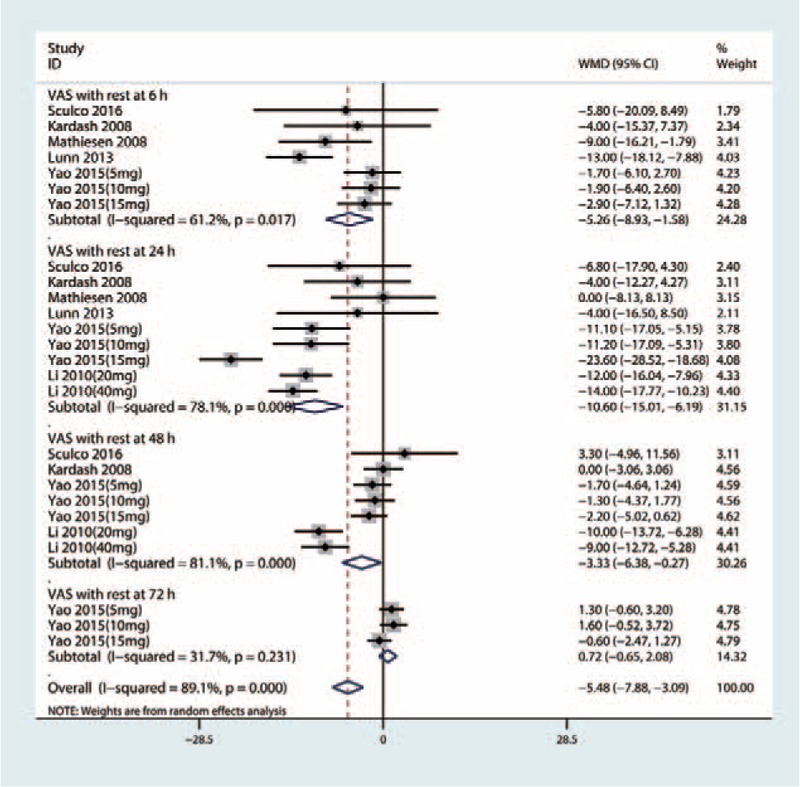
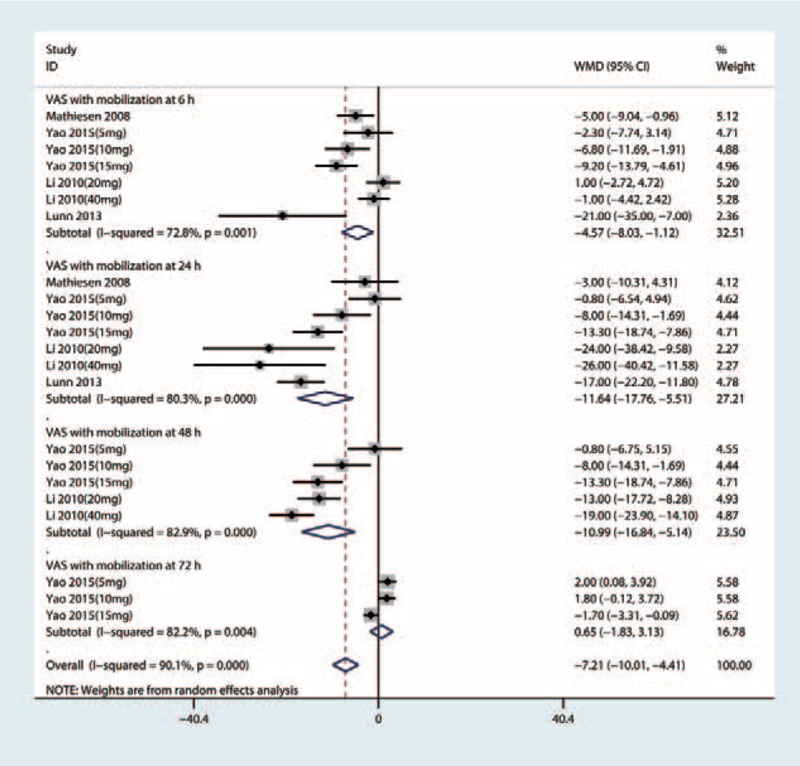
Methods: A computer literature search of electronic databases, including PubMed, Embase, the Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, China National Knowledge Infrastructure (CNKI), and China Wanfang database, was conducted to identify the relevant RCTs comparing preoperative intravenous glucocorticoids versus placebos for reducing acute pain and PONV in THA patients. The primary outcomes included the use of the visual analog scale (VAS) with rest or mobilization at 6, 24, 48, and 72 hours and the occurrence of PONV. The secondary outcome was total morphine consumption. We calculated the risk ratio (RR) with a 95% confidence interval (95% CI) for dichotomous outcomes, and the weighted mean difference (WMD) with a 95% CI for continuous outcomes.
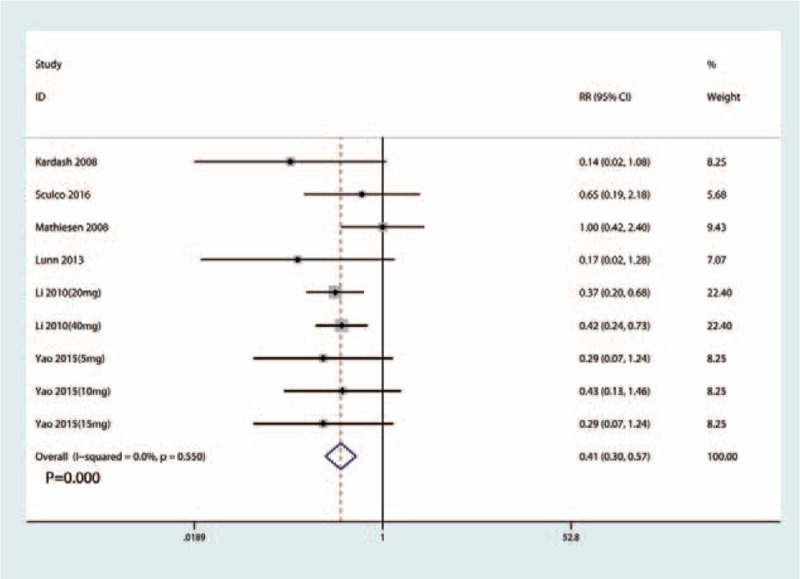
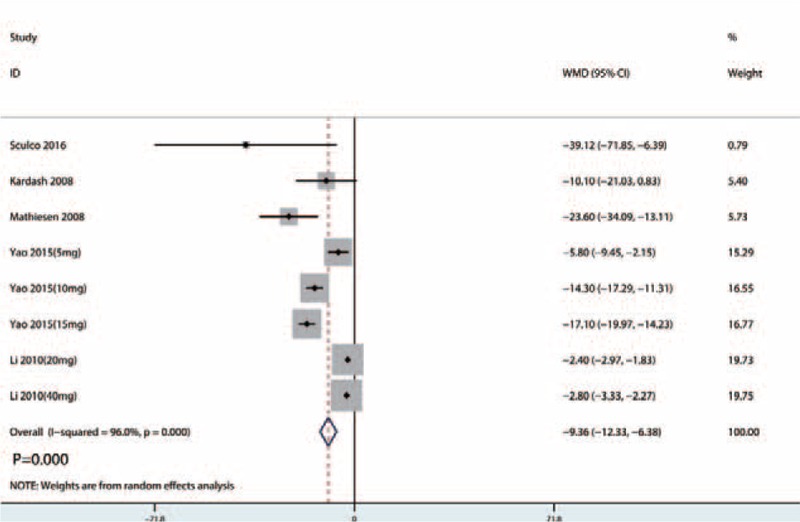
Results: Pooled data from 7 RCTs (411 THAs) favored preoperative intravenous glucocorticoids against acute pain intensity at 4, 24, and 48 hours (P < .05). There was no significant difference between the VAS with rest or mobilization at 72 hours (P > .05). Subsequently, preoperative intravenous glucocorticoids provided a total morphine-sparing effect of 9.36 mg (WMD = -9.36, 95% CI = -12.33 to -6.38, P = .000). In addition, preoperative intravenous glucocorticoids were associated with a significant reduction of the occurrence of PONV (RR = 0.41, 95% CI = 0.30-0.57, P = .000).
Conclusion: Intravenous glucocorticoids can decrease early pain intensity and PONV after THA. However, the low number of studies and variation in dosing regimens limits the evidence for its use. Thus, more high-quality RCTs are still needed to identify the optimal drug and the safety of intravenous glucocorticoids.
Copyright © 2017 The Authors. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Iorio R, Robb WJ, Healy WL, et al. Orthopaedic surgeon workforce and volume assessment for total hip and knee replacement in the United States: preparing for an epidemic. J Bone Joint Surg Am 2008;90:1598–605. - PubMed
-
- Lovald ST, Ong KL, Lau EC, et al. Mortality, cost, and downstream disease of total hip arthroplasty patients in the Medicare population. J Arthroplasty 2014;29:242–6. - PubMed
-
- Kurtz S, Ong K, Lau E, et al. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am 2007;89:780–5. - PubMed
-
- Macario A, Weinger M, Carney S, et al. Which clinical anesthesia outcomes are important to avoid? The perspective of patients. Anesth Analg 1999;89:652–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
