

Emphysematous change with scleroderma-associated interstitial lung disease: the potential contribution of vasculopathy?
- PMID: 29382307
- PMCID: PMC5791248
- DOI: 10.1186/s12890-018-0591-y
Emphysematous change with scleroderma-associated interstitial lung disease: the potential contribution of vasculopathy?
Abstract
Background: Pulmonary emphysema combined with systemic sclerosis (SSc)-associated interstitial lung disease (ILD) occurs more often in smokers but also in never-smokers. This study aimed to describe a new finding characterized by peculiar emphysematous change with SSc-associated ILD (SSc-ILD).
Methods: We conducted a retrospective review of 21 consecutive patients with SSc-ILD diagnosed by surgical lung biopsy and focused on the radio-pathological correlation of the emphysematous change.
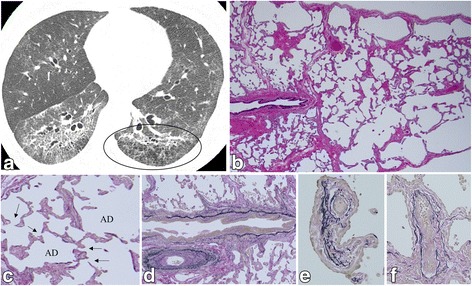
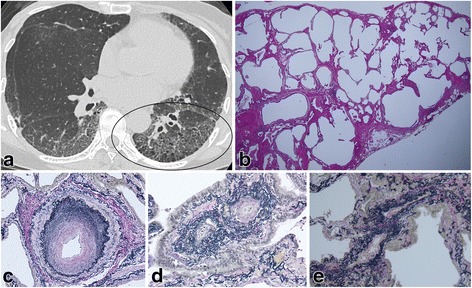
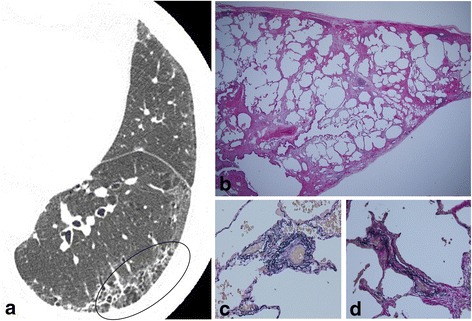
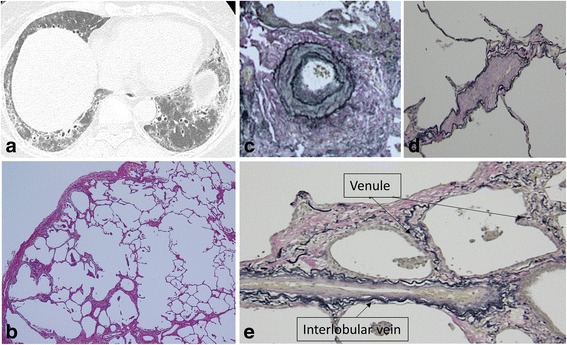
Results: Pathological pulmonary emphysema (p-PE) with SSc-ILD was the predominant complication in 16 patients (76.2%) with/without a smoking history, of whom 62.5% were never-smokers. A low attenuation area (LAA) within interstitial abnormality on high-resolution computed tomography (HRCT) was present in 31.3%. Diffusing capacity of the lung for carbon monoxide (DLCO) was lower, disease extent on HRCT higher, and intimal/medial thickening in muscular pulmonary arteries more common in the patients with p-PE with SSc-ILD. However, forced vital capacity (FVC) was well preserved regardless of whether p-PE was observed. Most SSc-ILD patients had pulmonary microvasculature changes in arterioles (90.5%), venules (85.7%), and interlobular veins (81.0%).
Conclusions: Pulmonary emphysematous changes (LAA within interstitial abnormalities on HRCT and destruction of fibrously thickened alveolar walls) are specific and novel radio-pathological features of SSc-ILD. Peripheral vasculopathy may help to destroy the fibrously thickened alveolar walls, resulting in emphysematous change in SSc-ILD.
Keywords: Emphysematous change; Systemic sclerosis; Vasculopathy.
Conflict of interest statement
Ethics approval and consent to participate
This retrospective cohort study was approved by the institutional review board of Kanagawa Cardiovascular and Respiratory Center (no. 28–11). The patients’ approval or informed consent was not required for a retrospective review of their records, pursuant to the ethical guidelines of the Japanese Ministry of Health, Labor, and Welfare.; however, the present retrospective study was carried out by the opt-out method of our hospital website.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Combined Pulmonary Fibrosis and Emphysema in Scleroderma-Related Lung Disease Has a Major Confounding Effect on Lung Physiology and Screening for Pulmonary Hypertension.Arthritis Rheumatol. 2016 Apr;68(4):1004-12. doi: 10.1002/art.39528. Arthritis Rheumatol. 2016. PMID: 26636545
-
Clinical Characteristics and Natural History of Autoimmune Forms of Interstitial Lung Disease: A Single-Center Experience.Lung. 2019 Dec;197(6):709-713. doi: 10.1007/s00408-019-00276-7. Epub 2019 Oct 3. Lung. 2019. PMID: 31583453
-
Performance of Forced Vital Capacity and Lung Diffusion Cutpoints for Associated Radiographic Interstitial Lung Disease in Systemic Sclerosis.J Rheumatol. 2018 Nov;45(11):1572-1576. doi: 10.3899/jrheum.171362. Epub 2018 Oct 1. J Rheumatol. 2018. PMID: 30275265 Free PMC article.
-
Predictors of progression in systemic sclerosis patients with interstitial lung disease.Eur Respir J. 2020 May 14;55(5):1902026. doi: 10.1183/13993003.02026-2019. Print 2020 May. Eur Respir J. 2020. PMID: 32079645 Free PMC article. Review.
-
Pulmonary function tests as outcomes for systemic sclerosis interstitial lung disease.Eur Respir Rev. 2018 May 15;27(148):170102. doi: 10.1183/16000617.0102-2017. Print 2018 Jun 30. Eur Respir Rev. 2018. PMID: 29769294 Free PMC article.
Cited by
-
Effect of combined pulmonary fibrosis and emphysema on patients with connective tissue diseases and systemic sclerosis: a systematic review and meta-analysis.Arthritis Res Ther. 2021 Apr 6;23(1):100. doi: 10.1186/s13075-021-02494-y. Arthritis Res Ther. 2021. PMID: 33823923 Free PMC article.
-
Syndrome of Combined Pulmonary Fibrosis and Emphysema: An Official ATS/ERS/JRS/ALAT Research Statement.Am J Respir Crit Care Med. 2022 Aug 15;206(4):e7-e41. doi: 10.1164/rccm.202206-1041ST. Am J Respir Crit Care Med. 2022. PMID: 35969190 Free PMC article.
-
Endothelial function and vascular events in patients with limited cutaneous systemic sclerosis (EFVELSS): a prospective observational study.Rheumatol Int. 2025 Jul 8;45(7):166. doi: 10.1007/s00296-025-05919-y. Rheumatol Int. 2025. PMID: 40627153 Free PMC article.
-
Emphysema formation in a never-smoker with scleroderma-related interstitial pneumonia.Respir Med Case Rep. 2018 Sep 13;25:211-212. doi: 10.1016/j.rmcr.2018.09.009. eCollection 2018. Respir Med Case Rep. 2018. PMID: 30237971 Free PMC article.
-
Combined Pulmonary Fibrosis and Emphysema: When Scylla and Charybdis Ally.Cells. 2023 Apr 28;12(9):1278. doi: 10.3390/cells12091278. Cells. 2023. PMID: 37174678 Free PMC article. Review.
References
-
- Desai SR, Veeraraghavan S, Hansell DM, Nikolakopolou A, Goh NS, Nicholson AG, et al. CT features of lung disease in patients with systemic sclerosis: comparison with idiopathic pulmonary fibrosis and nonspecific interstitial pneumonia. Radiology. 2004;232:560–567. doi: 10.1148/radiol.2322031223. - DOI - PubMed
-
- Kim DS, Yoo B, Lee JS, Kim EK, Lim CM, lee SD, et al. the major histopathologic pattern of pulmonary fibrosis in scleroderma is nonspecific interstitial pneumonia. Sarcoidosis Vasc Diffuse Lung Dis. 2002;19:121–127. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
