

The prevalence, burden and risk factors associated with chronic obstructive pulmonary disease in Commonwealth of Independent States (Ukraine, Kazakhstan and Azerbaijan): results of the CORE study
- PMID: 29382317
- PMCID: PMC5791247
- DOI: 10.1186/s12890-018-0589-5
The prevalence, burden and risk factors associated with chronic obstructive pulmonary disease in Commonwealth of Independent States (Ukraine, Kazakhstan and Azerbaijan): results of the CORE study
Abstract
Background: In the Commonwealth of Independent States (CIS) countries the epidemiology of chronic obstructive pulmonary disease (COPD) is poorly characterized. The objective of this analysis is to present the prevalence, burden and risk factors associated with COPD in three CIS countries as part of the CORE study (Chronic Obstructive Respiratory Diseases), the rationale and design of which have been described elsewhere.
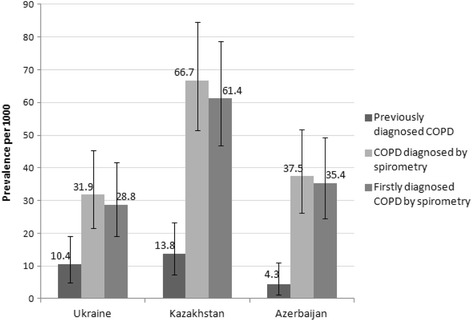
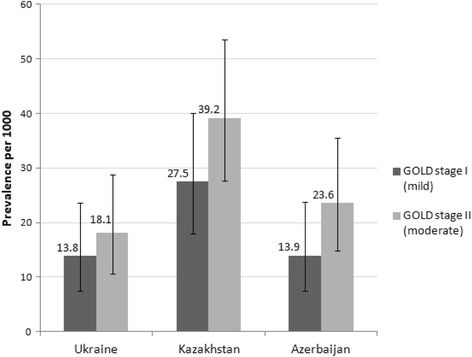
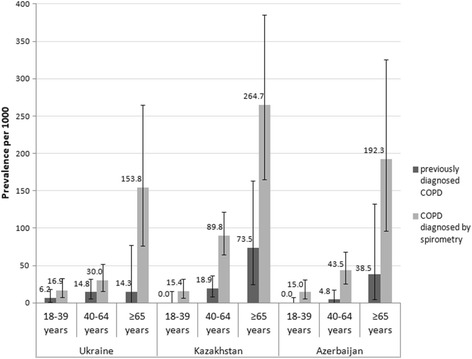
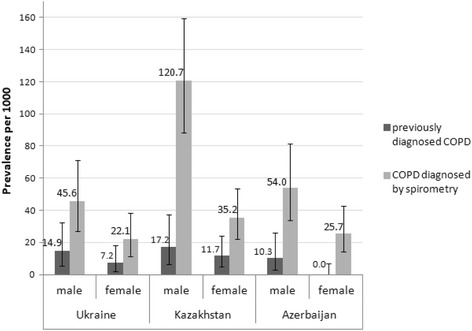
Methods: A total of 2842 adults (≥18 years) were recruited (964 in Ukraine, Kiev, 945 in Kazakhstan, Almaty and 933 in Azerbaijan, Baku) between 2013 and 2015 during household visits. Two-step cluster randomization was used for the sampling strategy. All respondents were interviewed about respiratory symptoms, smoking status and medical history, and underwent spirometry with bronchodilator. COPD was defined as (i) “previously diagnosed” when the respondent reported that he/she had previously been diagnosed with COPD by a doctor, (ii) “diagnosed by spirometry” using the GOLD criteria (2011) based on spirometry conducted during the study (FEV1/FVC < 0.70), and (iii) “firstly diagnosed by spirometry”, when the patient had received the COPD diagnosis for the first time based on the spirometry results obtained in this study.
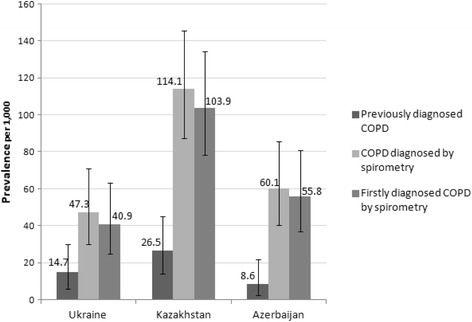
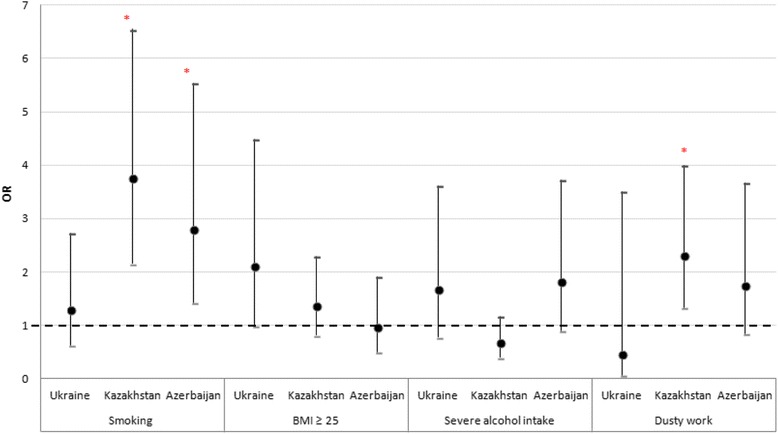
Results: The prevalence of “previously diagnosed” COPD was 10.4, 13.8 and 4.3 per 1000, and the prevalence of COPD “diagnosed by spirometry” was 31.9, 66.7 and 37.5 per 1000 in Ukraine, Kazakhstan, and Azerbaijan, respectively. Almost all respondents with COPD were diagnosed for the first time during this study. A statistically significant relationship was shown between smoking and COPD in Kazakhstan (odds ratio, OR: 3.75) and Azerbaijan (OR: 2.80); BMI in Ukraine (OR: 2.10); tuberculosis in Ukraine (OR: 32.3); and dusty work in Kazakhstan (OR: 2.30). Co-morbidities like cardiovascular diseases and a history of pneumonia occurred significantly (p < 0.05) more frequently in the COPD population compared to the non-COPD population across all participating countries. For hypertension, this was the case in Ukraine and Azerbaijan.
Conclusion: In CIS countries (Ukraine, Kazakhstan and Azerbaijan), the prevalence of COPD “diagnosed by spirometry” was significantly higher than the prevalence of previously diagnosed COPD. Compared to many other countries, the prevalence of COPD seems to be relatively low in CIS countries. Factors such as limited funding from the government; lack of COPD knowledge and the attitude within the population, and of primary care physicians; as well as low access to high-quality spirometry may play a role in this under-diagnosis of COPD. The information provided in this paper will be helpful for healthcare policy makers in CIS countries to instruct COPD management and prevention strategies and to allocate healthcare resources accordingly.
Keywords: Azerbaijan; Chronic obstructive pulmonary disease (COPD); Kazakhstan; Prevalence; Risk factors; Ukraine.
Conflict of interest statement
Ethics approval and consent to participate
The study was reviewed and approved by an Independent Ethics Committee in Kazakhstan (Central Commission for Ethics at the Ministry of Health of the Republic of Kazakhstan) and by Local Ethics Committees in Kazakhstan, Azerbaijan and Ukraine (Ethics Committee at Semey State Medical University, Almaty, Kazakhstan; Ethics Committee at Scientific Research Institute of Lung Diseases in Baku, Azerbaijan; Commission for Ethics at National Institute of Phthisiology and Pulmonology F.G. Yanovsky of NAMS, Kiev, Ukraine; Commission for Ethics at Center for Primary Health Care #2 of Shevchenko District, Kiev, Ukraine), according to the local legal requirements. Written informed consent was obtained from each participant before any procedures or data collection related to the study.
Consent for publication
Not applicable.
Competing interests
The study was sponsored by GlaxoSmithKline (GSK) marketing a number of treatments for COPD, Allergic Rhinitis, and Asthma.
DN, YF, LI, OG, EM, IA, NN report grants from GSK, during the conduct of the study; personal fees from GSK, outside the submitted work.
KM and JM are employees of GSK. AV and LT are GSK employees and shareholders.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Occupational Burden of Chronic Obstructive Pulmonary Disease in the Commonwealth of Independent States: Systematic Review and Meta-Analysis.Front Med (Lausanne). 2021 Jan 18;7:614827. doi: 10.3389/fmed.2020.614827. eCollection 2020. Front Med (Lausanne). 2021. PMID: 33537332 Free PMC article.
-
Chronic obstructive pulmonary disease, bronchial asthma and allergic rhinitis in the adult population within the commonwealth of independent states: rationale and design of the CORE study.BMC Pulm Med. 2017 Oct 10;17(1):131. doi: 10.1186/s12890-017-0471-x. BMC Pulm Med. 2017. PMID: 29017524 Free PMC article.
-
The prevalence, burden and risk factors associated with bronchial asthma in commonwealth of independent states countries (Ukraine, Kazakhstan and Azerbaijan): results of the CORE study.BMC Pulm Med. 2018 Jul 5;18(1):110. doi: 10.1186/s12890-018-0676-7. BMC Pulm Med. 2018. PMID: 29976177 Free PMC article.
-
Association between body mass index and patient-reported-outcome questionnaire scores (CAT™, ACT™, mMRC dyspnoea scale, IPAQ) in Ukraine, Kazakhstan and Azerbaijan: results of the CORE study.BMC Pulm Med. 2021 Jun 7;21(1):192. doi: 10.1186/s12890-021-01542-2. BMC Pulm Med. 2021. PMID: 34098922 Free PMC article.
-
Chronic obstructive pulmonary disease with mild airflow limitation: current knowledge and proposal for future research - a consensus document from six scientific societies.Int J Chron Obstruct Pulmon Dis. 2017 Aug 29;12:2593-2610. doi: 10.2147/COPD.S132236. eCollection 2017. Int J Chron Obstruct Pulmon Dis. 2017. PMID: 28919728 Free PMC article. Review.
Cited by
-
Occupational Burden of Chronic Obstructive Pulmonary Disease in the Commonwealth of Independent States: Systematic Review and Meta-Analysis.Front Med (Lausanne). 2021 Jan 18;7:614827. doi: 10.3389/fmed.2020.614827. eCollection 2020. Front Med (Lausanne). 2021. PMID: 33537332 Free PMC article.
-
Prevalence and Economic Burden of Respiratory Diseases in Central Asia and Russia: A Systematic Review.Int J Environ Res Public Health. 2020 Oct 14;17(20):7483. doi: 10.3390/ijerph17207483. Int J Environ Res Public Health. 2020. PMID: 33066700 Free PMC article.
-
Burden of Obstructive Lung Disease in Iran: Prevalence and Risk Factors for COPD in North of Iran.Int J Prev Med. 2020 Jul 3;11:78. doi: 10.4103/ijpvm.IJPVM_478_18. eCollection 2020. Int J Prev Med. 2020. PMID: 33033587 Free PMC article.
-
High COPD prevalence at high altitude: does household air pollution play a role?Eur Respir J. 2019 Feb 7;53(2):1801193. doi: 10.1183/13993003.01193-2018. Print 2019 Feb. Eur Respir J. 2019. PMID: 30464013 Free PMC article.
-
Prevalence and Risk Factors for COPD at High Altitude: A Large Cross-Sectional Survey of Subjects Living Between 2,100-4,700 m Above Sea Level.Front Med (Lausanne). 2020 Dec 3;7:581763. doi: 10.3389/fmed.2020.581763. eCollection 2020. Front Med (Lausanne). 2020. PMID: 33344472 Free PMC article.
References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–128. https://doi.org/10.1016/S0140-6736(12)61728-0. Erratum in: Lancet. 2013;381(9867):628. - DOI - PMC - PubMed
-
- Ignatiev VA, Titov OH, Gultyaeva OI. Chronic obstructive pulmonary disease: epidemiology and economic damage. Bulletin of St. Petersburg University. 2007; Issue 4: 37–46.
-
- Global Strategy for the Diagnosis, Management and Prevention of COPD [Revised 2011], Global Initiative for Chronic Obstructive Lung Disease. Accessed from: http://www.goldcopd.org April 2011 (GOLD 2011).
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
