

C-reactive protein for late-onset sepsis diagnosis in very low birth weight infants
- PMID: 29382319
- PMCID: PMC5791164
- DOI: 10.1186/s12887-018-1002-5
C-reactive protein for late-onset sepsis diagnosis in very low birth weight infants
Abstract
Background: Late-onset sepsis in very low birth weight (VLBW) infants is a diagnostic challenge. We aimed to evaluate the diagnostic utility of the C-Reactive protein (CRP) and the complete blood count (CBC) for late-onset sepsis in VLBW infants.
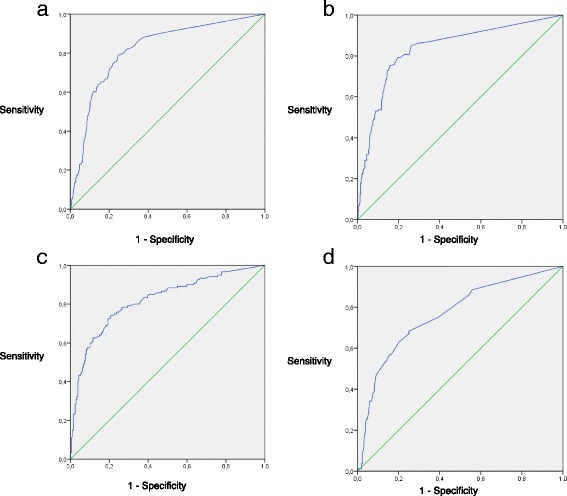
Methods: In a 5-year retrospective cohort of 416 VLBW infants born at less than 1500 g, there were 590 separate late-onset sepsis evaluations. CRP and CBC were drawn at time of initial blood culture (T0), at 16-24 h (T24) and 40-48 h (T48) after. The positive cut-off values for abnormal values were the following: CRP ≥10 mg/L and CBC with at least one anomaly, including white blood cell count < 5000/mm3, immature neutrophil/total neutrophil ratio > 0.10, or platelet count < 100,000/uL. Sensitivity and specificity for predicting late-onset sepsis were calculated for each laboratory test and their combinations. Receiver operating characteristics curves were obtained for each test and for the absolute change from T0 to T24 in the laboratory value of CRP, white blood cell count and immature neutrophil/total neutrophil.
Results: At T0, combining the CBC and the CRP had the highest sensitivity of 66% (95% confidence interval [CI], 58-73) compared to both individual tests for predicting late onset sepsis. At T24, CRP's sensitivity was 84% (95% CI, 78-89) and was statistically higher than the CBC's 59% (95% CI, 51-67). The combination of CBC at T0 and CRP at T24 offered the greatest sensitivity of 88% (95% CI, 82-92) and negative predictive value 93% (95% CI, 89-96), with fewer samples, compared to any other combination of tests. The area under the curve for the change in the white blood cell count from T0 to T24 was 0.82.
Conclusion: At initial sepsis evaluation (T0), both CBC and CRP should be performed to increase sensitivity. A highly negative predictive value is reachable with only two tests: a CBC at T0 and a CRP a T24.
Keywords: C-reactive protein; Late-onset sepsis; Neonatology; Very low birth weight.
Conflict of interest statement
Ethics approval and consent to participate
This study has been approved by the CHU de Québec Research and Ethics Board (REB). Permission to use the Med-Echo and TDR databases was obtained from Hospital Director and from CHU de Québec REB. Due to the retrospective design of the study using medical charts, individual patient consent was deemed unnecessary by the CHU de Québec REB.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
The cut-off levels of procalcitonin and C-reactive protein and the kinetics of mean platelet volume in preterm neonates with sepsis.BMC Pediatr. 2018 Aug 1;18(1):253. doi: 10.1186/s12887-018-1236-2. BMC Pediatr. 2018. PMID: 30068303 Free PMC article.
-
Diagnosis of late onset neonatal sepsis with cytokines, adhesion molecule, and C-reactive protein in preterm very low birthweight infants.Arch Dis Child Fetal Neonatal Ed. 1997 Nov;77(3):F221-7. doi: 10.1136/fn.77.3.f221. Arch Dis Child Fetal Neonatal Ed. 1997. PMID: 9462194 Free PMC article. Clinical Trial.
-
Can neutrophil responses in very low birth weight infants predict the organisms responsible for late-onset bacterial or fungal sepsis?J Perinatol. 2006 Aug;26(8):501-5. doi: 10.1038/sj.jp.7211554. Epub 2006 Jun 8. J Perinatol. 2006. PMID: 16761008
-
Procalcitonin versus C-reactive protein: review of kinetics and performance for diagnosis of neonatal sepsis.J Perinatol. 2019 Jul;39(7):893-903. doi: 10.1038/s41372-019-0363-4. Epub 2019 Mar 29. J Perinatol. 2019. PMID: 30926891 Review.
-
Assessment of C-Reactive Protein Diagnostic Test Accuracy for Late-Onset Infection in Newborn Infants: A Systematic Review and Meta-analysis.JAMA Pediatr. 2020 Mar 1;174(3):260-268. doi: 10.1001/jamapediatrics.2019.5669. JAMA Pediatr. 2020. PMID: 32011640 Free PMC article.
Cited by
-
Prediction modelling in the early detection of neonatal sepsis.World J Pediatr. 2022 Mar;18(3):160-175. doi: 10.1007/s12519-021-00505-1. Epub 2022 Jan 5. World J Pediatr. 2022. PMID: 34984642 Free PMC article. Review.
-
Assessment of a score's performance in predicting positive culture studies in preterm neonates with clinical suspicion of sepsis.J Mother Child. 2022 Apr 1;25(2):119-122. doi: 10.34763/jmotherandchild.20212502.d-21-00019. J Mother Child. 2022. PMID: 34786899 Free PMC article.
-
The Role of Coagulase-Negative Staphylococci Biofilms on Late-Onset Sepsis: Current Challenges and Emerging Diagnostics and Therapies.Antibiotics (Basel). 2023 Mar 10;12(3):554. doi: 10.3390/antibiotics12030554. Antibiotics (Basel). 2023. PMID: 36978421 Free PMC article. Review.
-
A study protocol for neonatal sepsis and gut microbiomics among preterm infants admitted at Muhimbili National Hospital, Tanzania.PLoS One. 2025 Jun 2;20(6):e0325099. doi: 10.1371/journal.pone.0325099. eCollection 2025. PLoS One. 2025. PMID: 40455875 Free PMC article.
-
Dependence of the severity of the systemic inflammatory response on resistance to hypoxia in male Wistar rats.J Inflamm Res. 2019 Mar 11;12:73-86. doi: 10.2147/JIR.S194581. eCollection 2019. J Inflamm Res. 2019. PMID: 30881082 Free PMC article.
References
-
- Fanaroff AA, Korones SB, Wright LL, Verter J, Poland RL, Bauer CR, et al. Incidence, presenting features, risk factors and significance of late onset septicemia in very low birth weight infants. The National Institute of Child Health and Human Development neonatal research network. Pediatr Infect Dis J. 1998;17(7):593–598. doi: 10.1097/00006454-199807000-00004. - DOI - PubMed
-
- Arnon S, Litmanovitz I, Regev R, Lis M, Shainkin-Kestenbaum R, Dolfin T. The prognostic virtue of inflammatory markers during late-onset sepsis in preterm infants. J Perinat Med. 2004;32(2):176–180. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
