

Pre-revascularization coronary wedge pressure as marker of adverse long-term left ventricular remodelling in patients with acute ST-segment elevation myocardial infarction
- PMID: 29382891
- PMCID: PMC5789971
- DOI: 10.1038/s41598-018-20276-6
Pre-revascularization coronary wedge pressure as marker of adverse long-term left ventricular remodelling in patients with acute ST-segment elevation myocardial infarction
Abstract
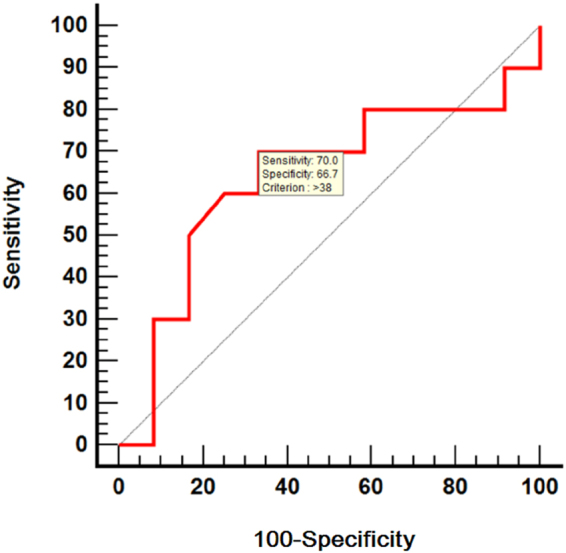
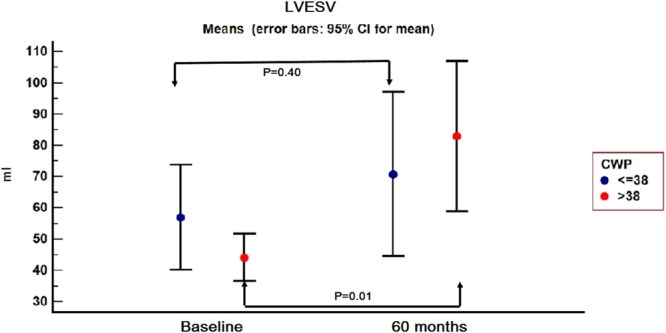
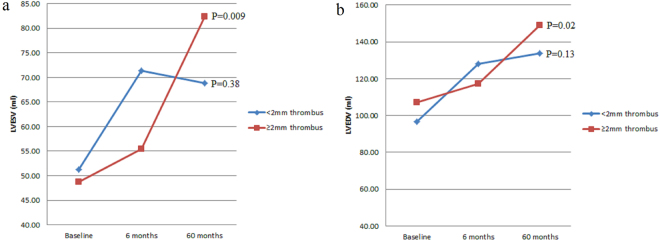
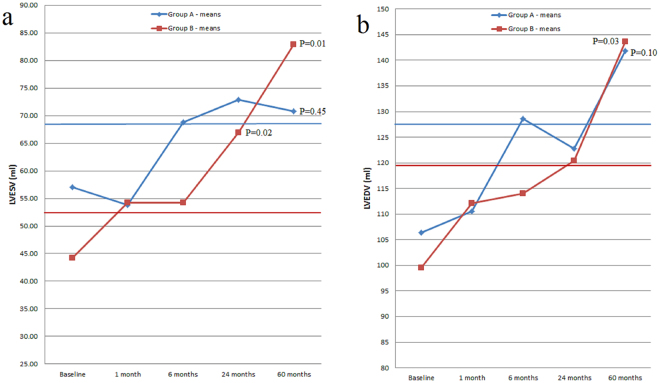
The aim of this study was to investigate the relationship between coronary wedge pressure (CWP), measured as a marker of pre-procedural microvascular obstruction, and left ventricular remodelling in high-risk ST-segment elevation myocardial infarction (STEMI) patients. Pre-revascularization CWP was measured in 25 patients with high-risk anterior STEMI. Left ventricular volumes and ejection fraction were echocardiographically measured at discharge and at follow-up. A 20% increase in left ventricular volumes was used to define remodelling. Patients with CWP ≤ 38 mmHg were characterized by late ventricular remodelling. Patients with CWP > 38 mmHg developed a progressive remodelling process which was associated with a significant 60 months increase in left ventricular volumes (P = 0.01 for end-systolic volume and 0.03 for end-diastolic volume) and a significant decrease in left ventricular ejection fraction (P = 0.05). A significant increase in both left ventricular end-systolic (P = 0.009) and end-diastolic volume (P = 0.02) from baseline to 60 months follow-up was recorded in patients with extracted thrombus length ≥2 mm. Pre-revascularization elevated CWP was associated with increased left ventricular volumes and decreased ejection fraction at long-term follow-up. CWP was a predictor of severe left ventricular enlargement, besides extracted thrombus quantity.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
In ST-segment elevation myocardial infarction, the echocardiographic parameters of microvascular obstruction are not associated with left ventricular remodeling at five years of follow-up.Echocardiography. 2019 Jun;36(6):1103-1109. doi: 10.1111/echo.14371. Epub 2019 May 22. Echocardiography. 2019. PMID: 31116460
-
Association between discharge heart rate and left ventricular adverse remodelling in ST segment elevation myocardial infarction patients treated with primary percutaneous coronary intervention.Heart. 2013 Apr;99(8):556-61. doi: 10.1136/heartjnl-2012-303406. Epub 2013 Mar 6. Heart. 2013. PMID: 23468514
-
Combined assessment of left ventricular end-diastolic pressure and ejection fraction by left ventriculography predicts long-term outcomes of patients with ST-segment elevation myocardial infarction.Heart Vessels. 2018 May;33(5):453-461. doi: 10.1007/s00380-017-1080-6. Epub 2017 Nov 15. Heart Vessels. 2018. PMID: 29143103
-
Mechanisms of myocardial reverse remodelling and its clinical significance: A scientific statement of the ESC Working Group on Myocardial Function.Eur J Heart Fail. 2024 Jul;26(7):1454-1479. doi: 10.1002/ejhf.3264. Epub 2024 Jun 4. Eur J Heart Fail. 2024. PMID: 38837573 Review.
-
Left Ventricular Remodelling: A Problem in Search of Solutions.Eur Cardiol. 2016 Aug;11(1):29-35. doi: 10.15420/ecr.2015:9:3. Eur Cardiol. 2016. PMID: 30310445 Free PMC article. Review.
Cited by
-
Renal Failure Impact on the Outcomes of ST-Segment Elevation Myocardial Infarction Patients Due to a Left Main Coronary Culprit Lesion Treated Using a Primary Percutaneous Coronary Intervention.J Clin Med. 2019 Apr 25;8(4):565. doi: 10.3390/jcm8040565. J Clin Med. 2019. PMID: 31027307 Free PMC article.
-
Optical Coherence Tomography for In Vivo Identification, Characterization and Optimal Treatment of Spontaneous Recanalization of Coronary Thrombus.In Vivo. 2020 Mar-Apr;34(2):745-756. doi: 10.21873/invivo.11834. In Vivo. 2020. PMID: 32111780 Free PMC article.
-
Coronary Microcirculation: The Next Frontier in the Management of STEMI.J Clin Med. 2023 Feb 17;12(4):1602. doi: 10.3390/jcm12041602. J Clin Med. 2023. PMID: 36836137 Free PMC article. Review.
-
Distinctive Morphological Patterns of Complicated Coronary Plaques in Acute Coronary Syndromes: Insights from an Optical Coherence Tomography Study.Diagnostics (Basel). 2022 Nov 17;12(11):2837. doi: 10.3390/diagnostics12112837. Diagnostics (Basel). 2022. PMID: 36428897 Free PMC article.
-
Predilation Ballooning in High Thrombus Laden STEMIs: An Independent Predictor of Slow Flow/No-Reflow in Patients Undergoing Emergent Percutaneous Coronary Revascularization.J Interv Cardiol. 2023 Jan 6;2023:4012361. doi: 10.1155/2023/4012361. eCollection 2023. J Interv Cardiol. 2023. PMID: 36712997 Free PMC article.
References
-
- Hamirani YS, Wong A, Kramer CM, Salerno M. Effect of microvascular obstruction and intramyocardial haemorrhage by CMR on LV remodelling and outcomes after myocardial infarction: a systematic review and meta-analysis. J. Am. Coll. Cardiol. Img. 2014;7:940–952. doi: 10.1016/j.jcmg.2014.06.012. - DOI - PMC - PubMed
-
- Eitel I, et al. Intracoronary Compared With Intravenous Bolus Abciximab Application During Primary Percutaneous Coronary Intervention in ST-Segment Elevation Myocardial Infarction: Cardiac Magnetic Resonance Substudy of the AIDA STEMI Trial. J. Am. Coll. Cardiol. 2014;61:1447–1454. doi: 10.1016/j.jacc.2013.01.048. - DOI - PubMed
-
- Patel N, et al. Zero-Flow Pressure Measured Immediately After Primary Percutaneous Coronary Intervention for ST-Segment Elevation Myocardial Infarction Provides the Best Invasive Index for Predicting the Extent of Myocardial Infarction at 6 Months: An OxAMI Study (Oxford Acute Myocardial Infarction) J. Am. Coll. Cardiol. Intv. 2015;8:1410–1421. doi: 10.1016/j.jcin.2015.04.029. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
