

Chronic Recurrent Temporomandibular Joint Dislocation: A Comparison of Various Surgical Treatment Options, and Demonstration of the Versatility and Efficacy of the Dautrey's Procedure
- PMID: 29383002
- PMCID: PMC5772030
- DOI: 10.1007/s12663-017-1019-6
Chronic Recurrent Temporomandibular Joint Dislocation: A Comparison of Various Surgical Treatment Options, and Demonstration of the Versatility and Efficacy of the Dautrey's Procedure
Abstract
Introduction: There has been a changing trend of treating temporomandibular joint subluxation, which range from conservative non-surgical measures to various soft and hard tissue surgical procedures aimed at either augmenting or restricting the condylar path.
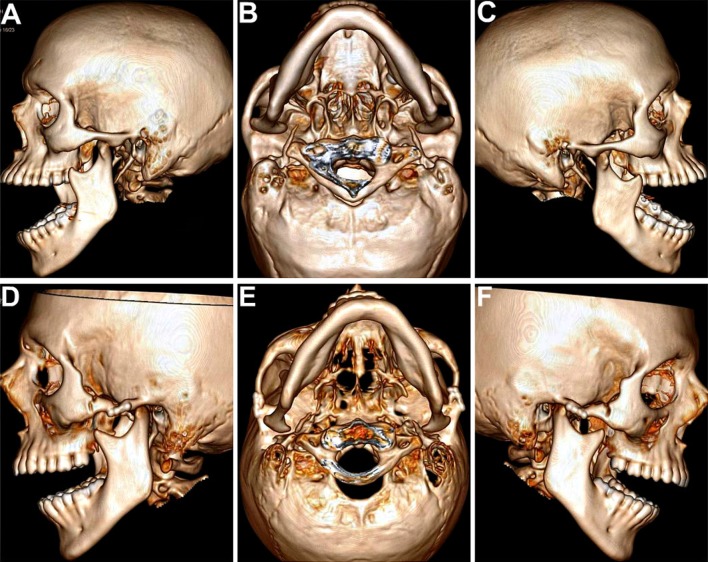
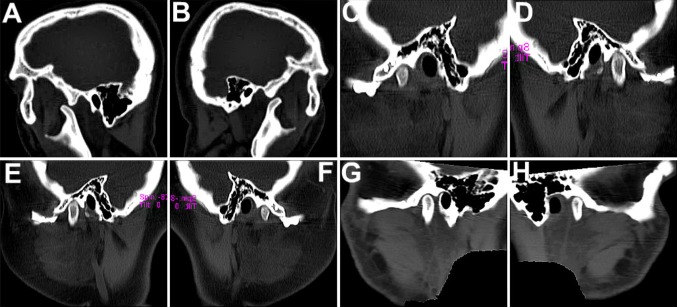
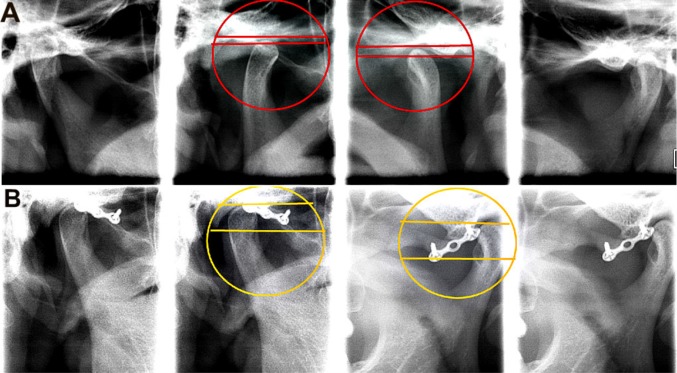
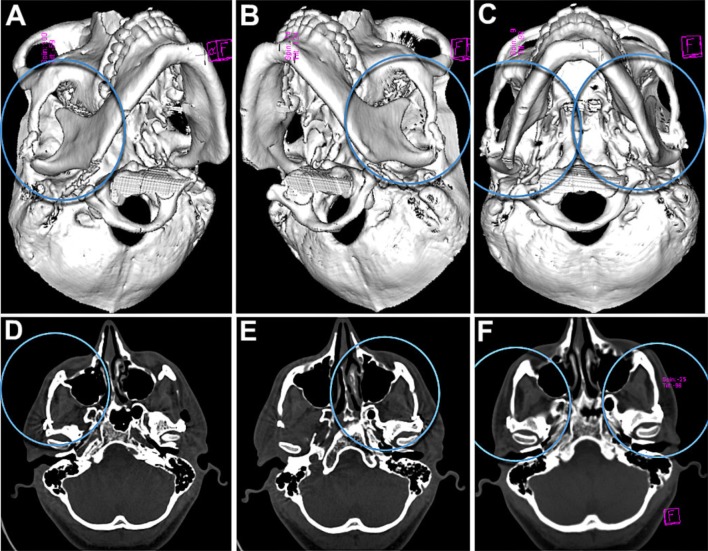
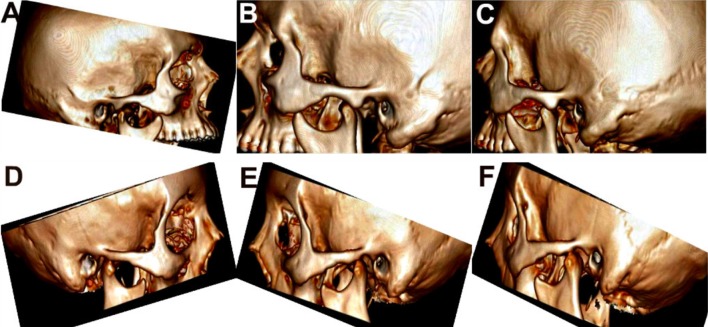
Aim: This study was aimed at comparing the efficacy of three major surgical treatment modalities: condylar obstruction creation, obstruction removal and anti-translatory procedures. Also, the location, anatomy and morphology of the TMJs pre- and post-surgery were evaluated and compared using radiographs, sagittal and 3-D Computed Tomographic scans.
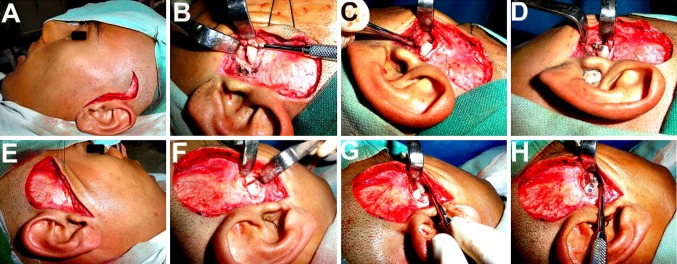
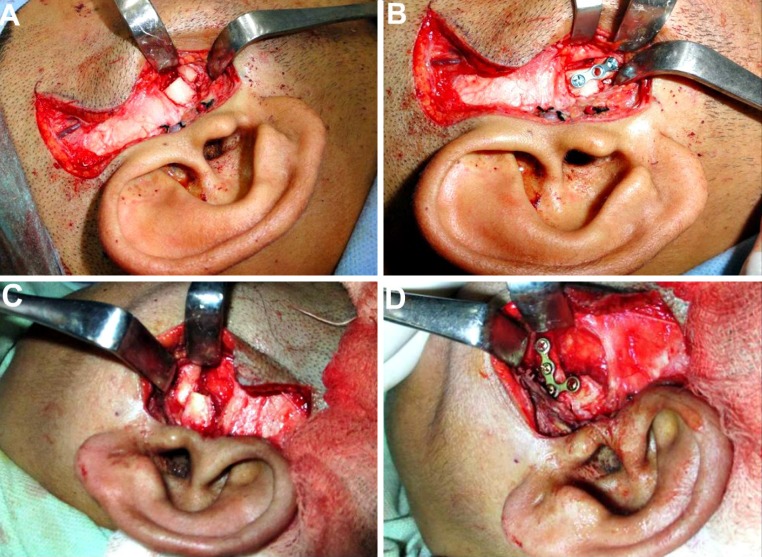
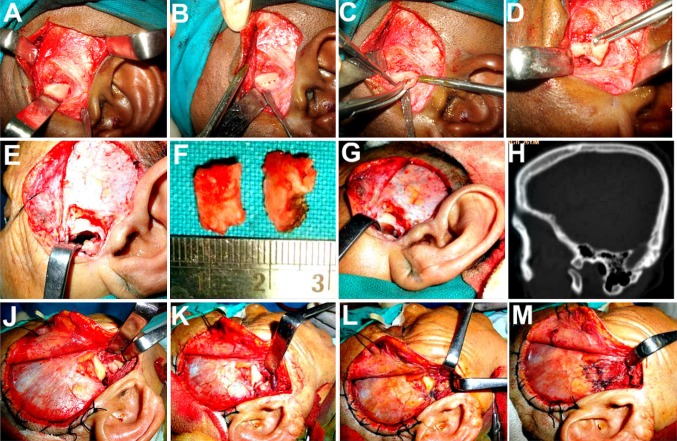
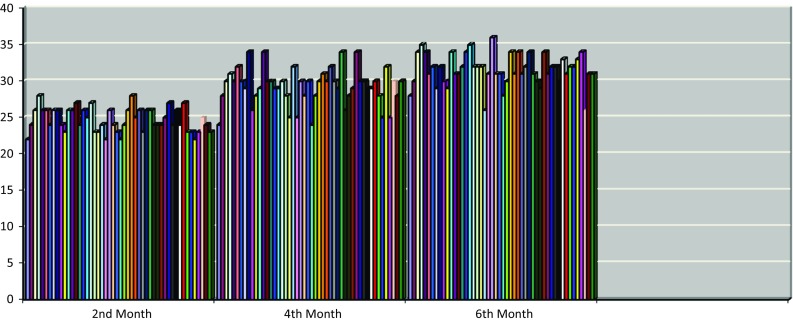
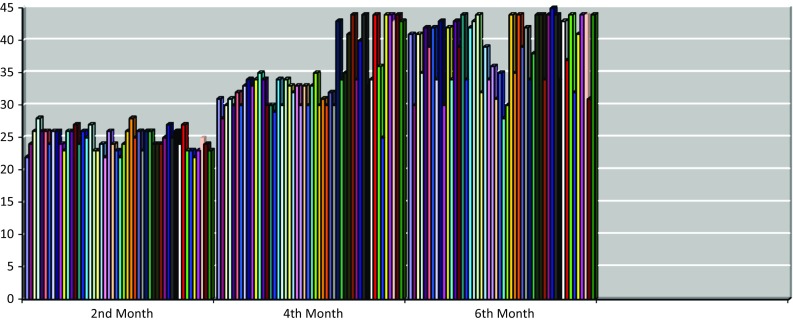
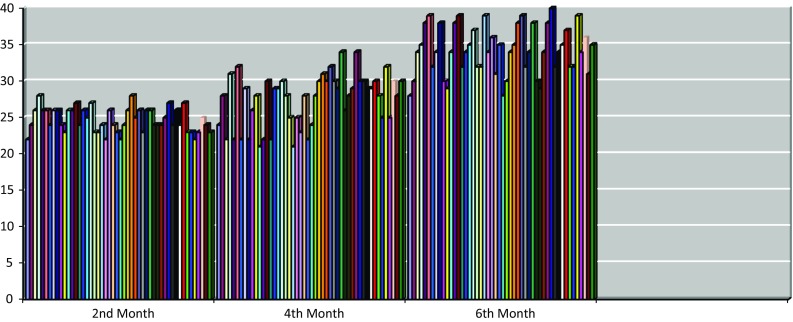
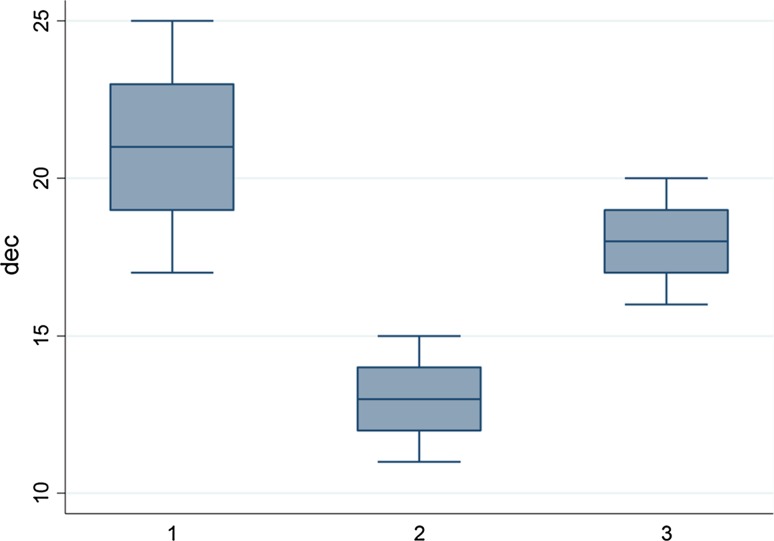
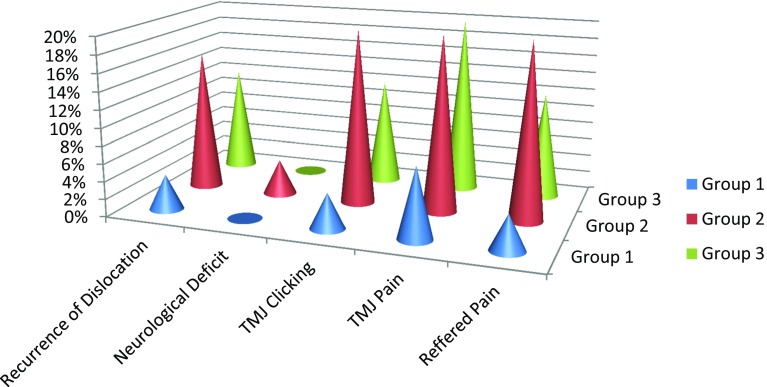
Materials and methods: A 6-year study was carried out on seventy-five patients of various age groups. Twenty-five were operated by the Dautrey's procedure, 25 by articular eminectomy alone and the remaining 25 by eminectomy followed by meniscal plication and tethering. The distribution of patients in the three groups was random. Effectiveness of the surgical procedure and incidence of complications including recurrence were carefully compiled and compared between the three groups.
Results and conclusion: Dautrey's procedure yielded more gratifying and stable results, leading to a successful and permanent correction of chronic recurrent dislocation of the TMJs, with practically nil complications, thus demonstrating it to be an extremely safe, effective and versatile technique, making the joints function normally and securing sufficient volume of mouth opening. There was observed an average increase in articular tubercle height by 3.65 mm and a mean anterior shift of its lowest point by 4.5 mm following the Dautrey's procedure, which were statistically significant findings. The upper age limit to carry out the Dautrey's procedure can be safely taken up to 45 years.
Keywords: Arthroplasty; Capsulorrhaphy; Dautrey’s procedure; Eminectomy; Hypermobility; Meniscal plication; Subluxation.
Conflict of interest statement
Compliance with Ethical StandardsThe author of this article has not received any research grant, remuneration, or speaker honorarium from any company or committee whatsoever, and neither owns any stock in any company. The author declares that she does not have any conflict of interest.All procedures performed on the patients (human participants) involved were in accordance with the ethical standards of the institution and/or national research committee, as well as with the 1964 Helsinki declaration and its later amendments and comparable ethical standards.This article does not contain any new studies with human participants or animals performed by the author.Informed consent was obtained from all the individual participants in this study.
Figures
References
-
- Helman J, Laufer D, Minkov B, Gutman D. Eminectomy as surgical treatment for chronic mandibular dislocations. Int J Oral Surg. 1984;47:179–184. - PubMed
-
- Bhandari S, Swain M, Dewoolkar LV. Temporomandibular joint dislocation after laryngeal mask airway insertion. Internet J Anesthesiol. 2008;16:1–4.
LinkOut - more resources
Full Text Sources
Other Literature Sources