

Vonoprazan fumarate, a novel potassium-competitive acid blocker, in the management of gastroesophageal reflux disease: safety and clinical evidence to date
- PMID: 29383028
- PMCID: PMC5784563
- DOI: 10.1177/1756283X17745776
Vonoprazan fumarate, a novel potassium-competitive acid blocker, in the management of gastroesophageal reflux disease: safety and clinical evidence to date
Abstract
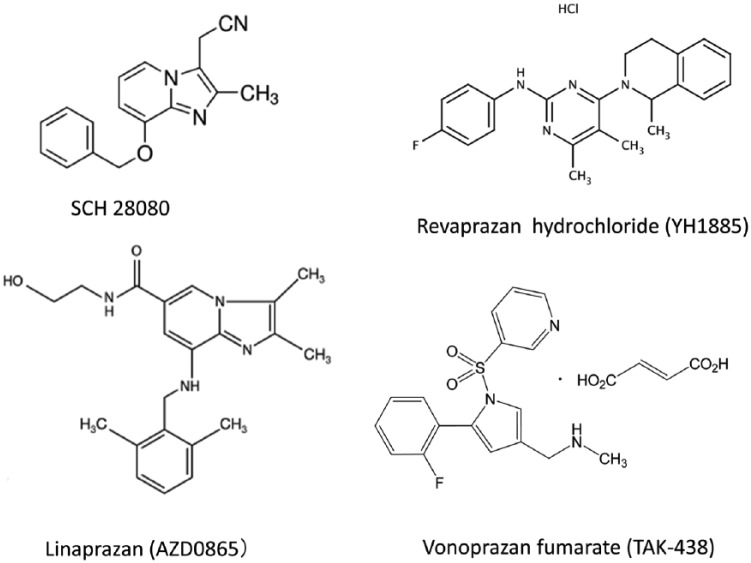
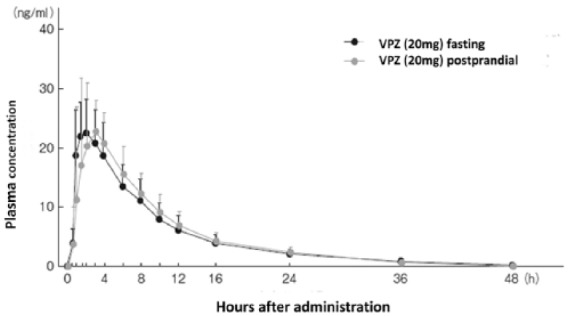
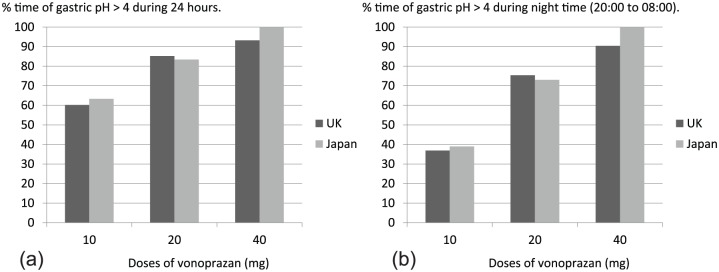
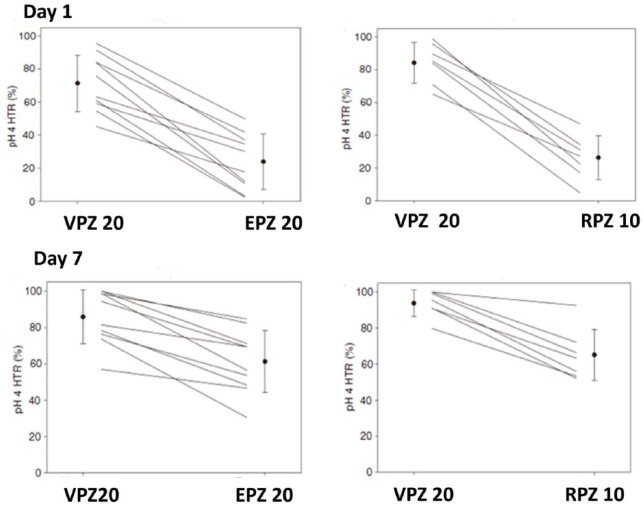
Potassium-competitive acid blocker (P-CAB) is a class of drug that competitively blocks the potassium-binding site of H+, K+-adenosine triphosphate (ATP)ase. Although the history of this class of drugs started over 30 years ago, clinical use of two P-CABs, revaprazan and vonoprazan, were only recently approved in Korea and Japan, respectively. Among them, vonoprazan has several advantages over conventional proton-pump inhibitors (PPIs), including rapid onset of action, long duration of acid suppression, fewer interindividual variations in terms of acid suppression, and minimum dietary influence on its action. These advantages of vonoprazan have been proved in clinical trials conducted for license approvals for several acid-related diseases. In this review article, current evidence of vonoprazan in the management of gastroesophageal reflux disease (GERD) will be summarized. Since the clinical trial data, as well as postmarketed clinical data, have consistently demonstrated superiority of vonoprazan over conventional PPIs in terms of achieving healing of mucosal breaks and maintaining the healing, it may provide an excellent, if not complete, option for fulfilling some of the unmet needs for current GERD therapy. The safety problem of vonoprazan is also discussed, as more pronounced hypergastrinemia inevitably ensues with its use.
Keywords: gastroesophageal reflux disease; potassium-competitive acid blocker; proton pump inhibitor; safety; vonoprazan.
Conflict of interest statement
Conflict of interest statement: KS has received lecture fees from Takeda Pharma Inc., EA Pharma and Astra Zeneca.
Figures
References
-
- Fock KM, Talley N, Goh KL, et al. Asia-Pacific consensus on the management of gastro-oesophageal reflux disease: an update focusing on refractory reflux disease and Barrett’s oesophagitis. Gut 2016; 65: 1402–1415. - PubMed
-
- Kinoshita Y, Adachi K, Hongo M, et al. Systematic review of the epidemiology of gastroesophageal reflux disease in Japan. J Gastroenterol 2011; 46: 1092–1103. - PubMed
-
- Richter JE, Kahrilas PJ, Johanson J, et al. Efficacy and safety of esomeprazole compared with omeprazole in GERD patients with erosive esophagitis: a randomized controlled trial. Am J Gastroenterol 2001; 96: 656–665. - PubMed
-
- Sifrim D, Zerbib F. Diagnosis and management of patients with reflux symptoms refractory to proton pump inhibitors. Gut 2012; 61: 1340–1354. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
