

Radiation effects on antitumor immune responses: current perspectives and challenges
- PMID: 29383033
- PMCID: PMC5784573
- DOI: 10.1177/1758834017742575
Radiation effects on antitumor immune responses: current perspectives and challenges
Abstract
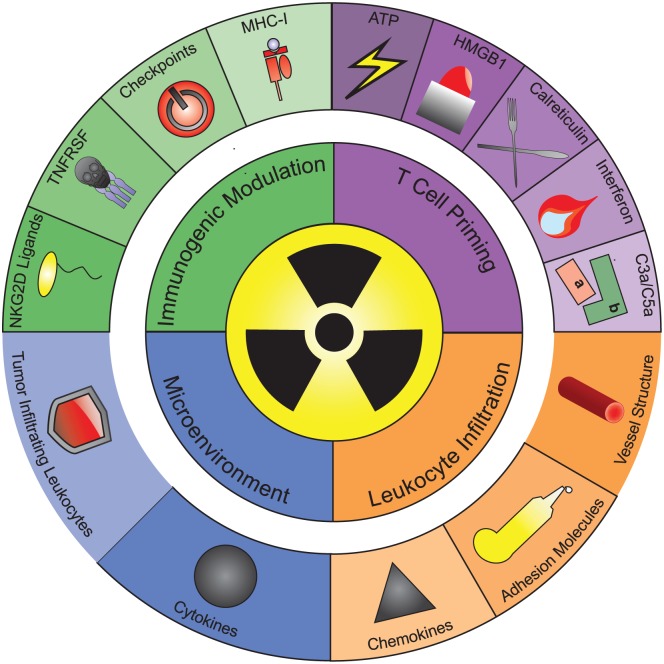
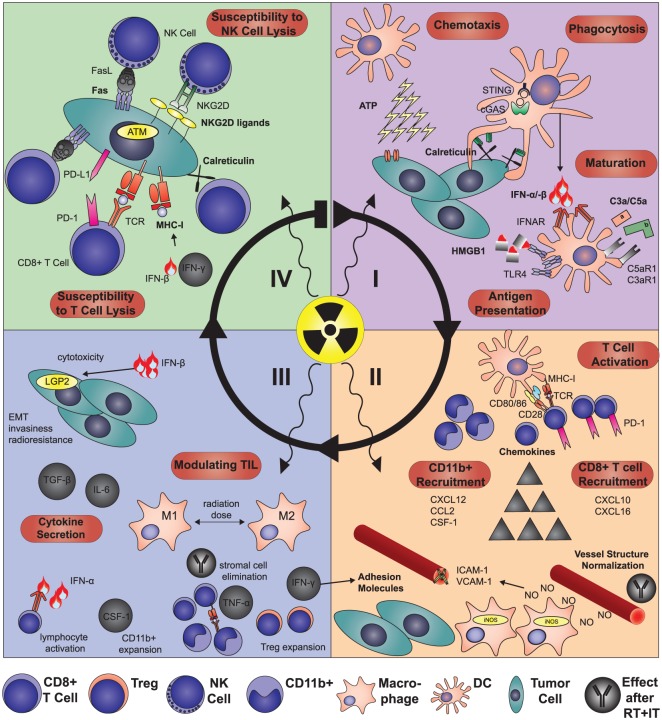
Radiotherapy (RT) is currently used in more than 50% of cancer patients during the course of their disease in the curative, adjuvant or palliative setting. RT achieves good local control of tumor growth, conferring DNA damage and impacting tumor vasculature and the immune system. Formerly regarded as a merely immunosuppressive treatment, pre- and clinical observations indicate that the therapeutic effect of RT is partially immune mediated. In some instances, RT synergizes with immunotherapy (IT), through different mechanisms promoting an effective antitumor immune response. Cell death induced by RT is thought to be immunogenic and results in modulation of lymphocyte effector function in the tumor microenvironment promoting local control. Moreover, a systemic immune response can be elicited or modulated to exert effects outside the irradiation field (so called abscopal effects). In this review, we discuss the body of evidence related to RT and its immunogenic potential for the future design of novel combination therapies.
Keywords: PD-1; abscopal; brachytherapy; checkpoint inhibitors; immunogenic cell death; immunotherapy; radiotherapy.
Conflict of interest statement
Conflict of interest statement: IM has received research support and personal fees from Bristol-Myers Squibb, Roche, AstraZeneca, Bayer, Lilly, Genmab, Incyte, Alligator, Merck-Serono, Pfizer, MSD. The rest of the authors declare no conflicts of interest.
Figures
References
-
- Wara WM. Immunosuppression associated with radiation therapy. Int J Radiat Oncol Biol Phys 1977; 2: 593–596. - PubMed
-
- Demaria S, Ng B, Devitt ML, et al. Ionizing radiation inhibition of distant untreated tumors (abscopal effect) is immune mediated. Int J Radiat Oncol Biol Phys 2004; 58: 862–870. - PubMed
-
- Rodriguez-Ruiz ME, Rodriguez I, Garasa S, et al. Abscopal effects of radiotherapy are enhanced by combined immunostimulatory mAbs and are dependent on CD8 T cells and crosspriming. Cancer Res 2016; 76: 5994–6005. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
