

Optimal Intereye Difference Thresholds in Retinal Nerve Fiber Layer Thickness for Predicting a Unilateral Optic Nerve Lesion in Multiple Sclerosis
- PMID: 29384802
- PMCID: PMC8845082
- DOI: 10.1097/WNO.0000000000000629
Optimal Intereye Difference Thresholds in Retinal Nerve Fiber Layer Thickness for Predicting a Unilateral Optic Nerve Lesion in Multiple Sclerosis
Abstract
Background: The optic nerve is a frequent site for involvement in multiple sclerosis (MS). Optical coherence tomography (OCT) detects thinning of the retinal nerve fiber layer (RNFL) in eyes of patients with MS and in those meeting criteria for clinically or radiologically isolated demyelinating syndromes. Current international diagnostic criteria for MS do not include the optic nerve as an imaging lesion site despite the high prevalence of acute optic neuritis (ON), or occult optic neuropathy, among early MS and clinically isolated syndrome patients; as well as most MS patients over the course of the disease. We sought to determine optimal thresholds for intereye difference in peripapillary RNFL thickness that are most predictive of a unilateral optic nerve lesion.
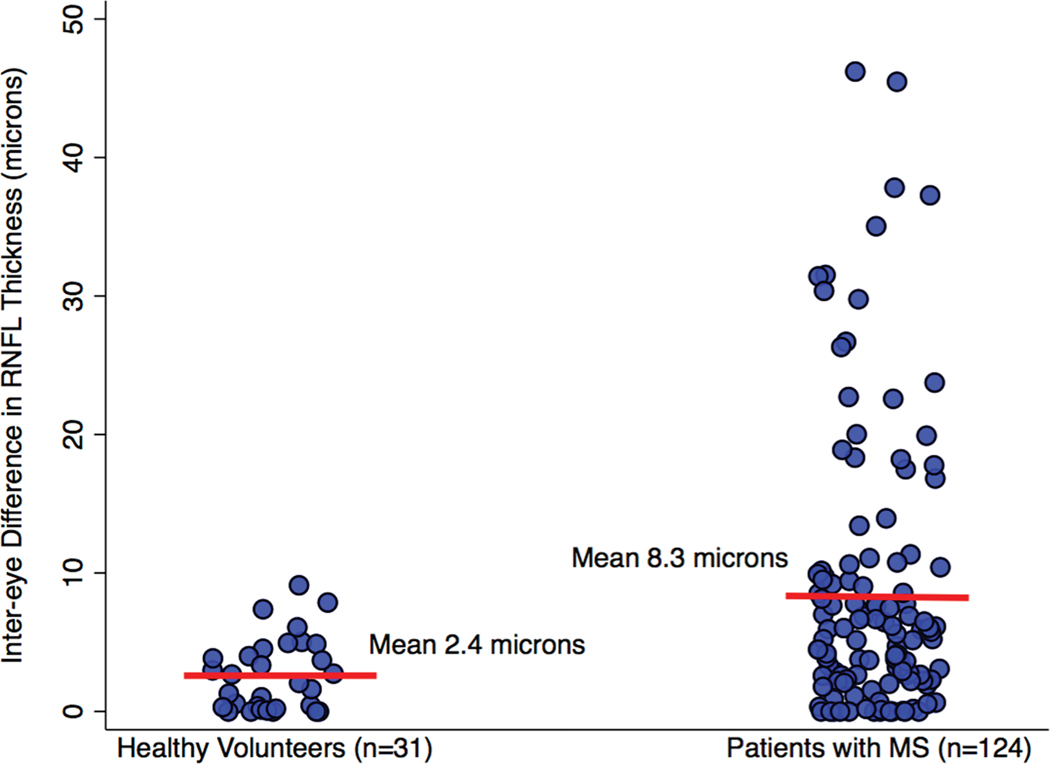
Methods: We analyzed spectral domain OCT data of 31 healthy volunteers and 124 patients with MS at a single center as part of an ongoing collaborative investigation of visual outcomes. Intereye differences in peripapillary (360°) RNFL thickness were calculated as the absolute value of the difference. First, we determined the 95th percentile value of intereye difference for the healthy volunteers. This value was applied to the convenience sample group of MS patients as a validation cohort determining how well this threshold could distinguish patients with vs without a history of unilateral ON. The relation of intereye differences in peripapillary RNFL thickness to binocular low-contrast letter acuity scores was also examined.
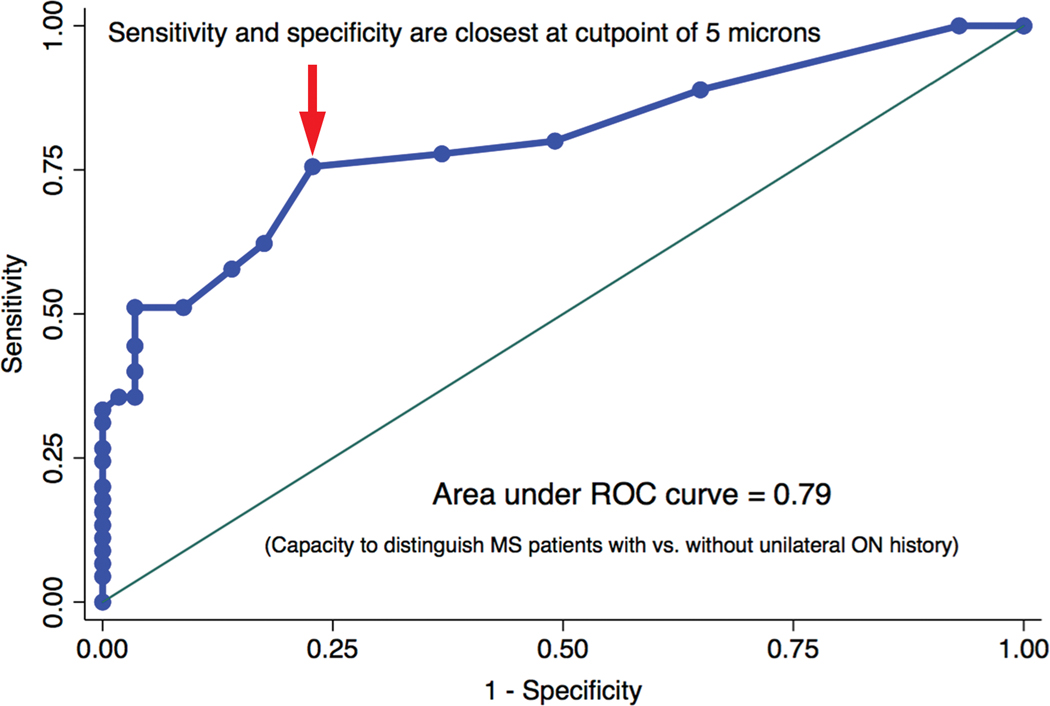
Results: Among healthy volunteer participants (n = 31), the 95th percentile value for intereye difference (upper boundary of expected for normal controls) was 6.0 μm. This value was applied to the convenience sample group of MS patients (n = 124, validation cohort). Positive predictive value, negative predictive value, sensitivity, and specificity for identifying MS patients with a history of unilateral ON were calculated for the 6-μm threshold value in a 2 × 2 table analysis with the application of χ tests (P < 0.0001). The 6-μm threshold was predictive of worse binocular low-contrast acuity scores at 2.5% (P = 0.03) and 1.25% (P = 0.002 by linear regression analyses). A receiver operating characteristic curve analysis demonstrated an optimal intereye difference threshold of 5 μm for identifying unilateral ON in the MS cohort.
Conclusions: An intereye difference of 5-6 μm in RNFL thickness is a robust structural threshold for identifying the presence of a unilateral optic nerve lesion in MS.
Figures
References
-
- Sorensen TL, Frederiksen JL, Bronnum-Hansen H, Petersen HC. Optic neuritis as onset manifestation of multiple sclerosis: a nationwide, long-term survey. Neurology. 1999;53:473–478. - PubMed
-
- Balcer LJ. Clinical practice. Optic neuritis. N Engl J Med. 2006;354:1273–1280. - PubMed
-
- Foroozan R, Buono LM, Savino PJ, Sergott RC. Acute demyelinating optic neuritis. Curr Opin Ophthalmol. 2002;13:375–380. - PubMed
-
- Frohman EM, Frohman TC, Zee DS, McColl R, Galetta S. The neuro-ophthalmology of multiple sclerosis. Lancet Neurol. 2005;4:111–121. - PubMed
-
- Arnold AC. Evolving management of optic neuritis and multiple sclerosis. Am J Ophthalmol. 2005;139:1101–1108. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
