

Comparison of the clinical effects of zero-profile anchored spacer (ROI-C) and conventional cage-plate construct for the treatment of noncontiguous bilevel of cervical degenerative disc disease (CDDD): A minimum 2-year follow-up
- PMID: 29384883
- PMCID: PMC5805455
- DOI: 10.1097/MD.0000000000009808
Comparison of the clinical effects of zero-profile anchored spacer (ROI-C) and conventional cage-plate construct for the treatment of noncontiguous bilevel of cervical degenerative disc disease (CDDD): A minimum 2-year follow-up
Abstract
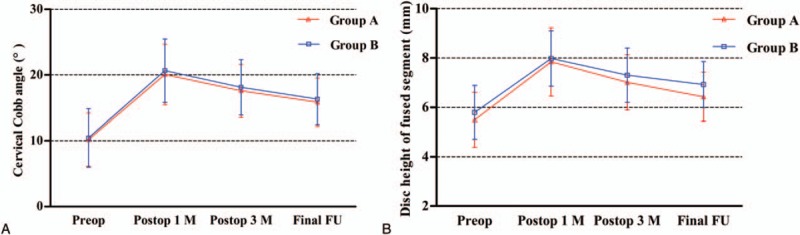
Comparing the clinical and radiographic outcomes in anterior cervical discectomy and fusion (ACDF) using a zero-profile anchored spacer (ROI-C) or a conventional cage-plate construct (CPC) for treating noncontiguous bilevel of cervical degenerative disc disease (CDDD).Overall, 46 patients with 2 noncontiguous segments of CDDD, treated with ACDF from January 2011 to October 2015, were included in this study. ROI-C was used in 22 patients (group A) and CPC in 24 patients (group B). The clinical and radiographic outcomes and complications were compared pre- and postoperatively. All patients were followed up for at least 24 months after surgery.No significant difference was found in fusion rate, cervical curvature, height of fused segment (FSDH), intraoperative blood loss, and Japanese Orthopaedic Association (JOA), and Neck Disability Index (NDI) scores between the 2 groups. Group A had a shorter operation time and significantly lower incidence of dysphagia (3 and 24 months postoperatively) than group B (P < .001 and P < .05, respectively). Moreover, group A had a higher loss of FSDH than group B, but with no difference between the 2 groups (P > .05). Two cages developed subsidence in group A (4.5%) and 2 adjacent levels developed degeneration in group B (2,8%).ACDF with ROI-C device was superior to CPC for noncontiguous bilevel of CDDD because it avoided postoperative dysphagia and required a shorter operation time. Moreover, the clinical outcomes were comparable. Prospective trials with larger samples and longer follow-up are required to confirm the results.
Conflict of interest statement
The authors report no conflicts of interest.
Figures




References
-
- Fountas KN, Kapsalaki EZ, Nikolakakos LG, et al. Anterior cervical discectomy and fusion associated complications. Spine (Phila Pa 1976) 2007;32:2310–7. - PubMed
-
- Fraser JF, Härtl R. Anterior approaches to fusion of the cervical spine: a metaanalysis of fusion rates. J Neurosurg Spine 2007;6:298–303. - PubMed
-
- Mobbs RJ, Rao P, Chandran NK. Anterior cervical discectomy and fusion: analysis of surgical outcome with and without plating. J Clin Neurosci 2007;14:639–42. - PubMed
-
- Song KJ, Taghavi CE, Lee KB, et al. The efficacy of plate construct augmentation versus cage alone in anterior cervical fusion. Spine (Phila Pa 1976) 2009;34:2886–92. - PubMed
-
- Bazaz R, Lee MJ, Yoo JU. Incidence of dysphagia after anterior cervical spine surgery: a prospective study. Spine (Phila Pa 1976) 2002;27:2453–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
