

Multiple cerebral gliomas mimicking central nervous system inflammatory demyelinating diseases: A rare case with review of literature
- PMID: 29384930
- PMCID: PMC6392929
- DOI: 10.1097/MD.0000000000009456
Multiple cerebral gliomas mimicking central nervous system inflammatory demyelinating diseases: A rare case with review of literature
Abstract
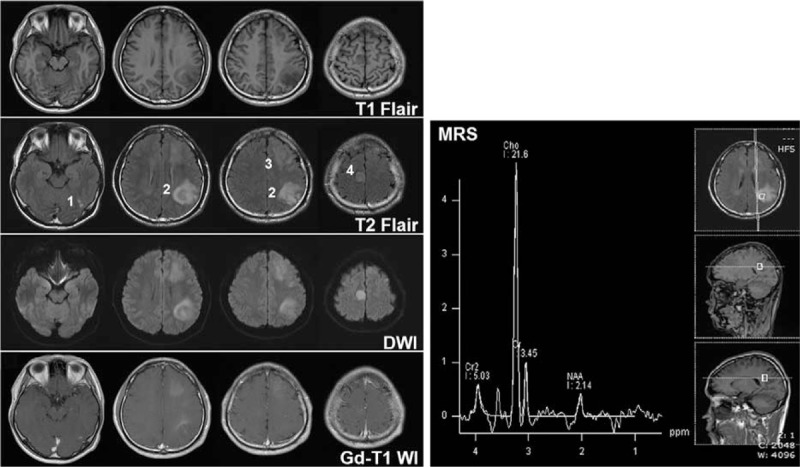
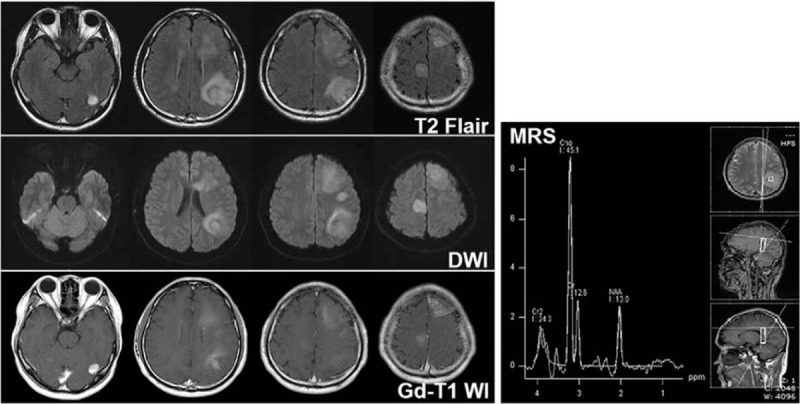
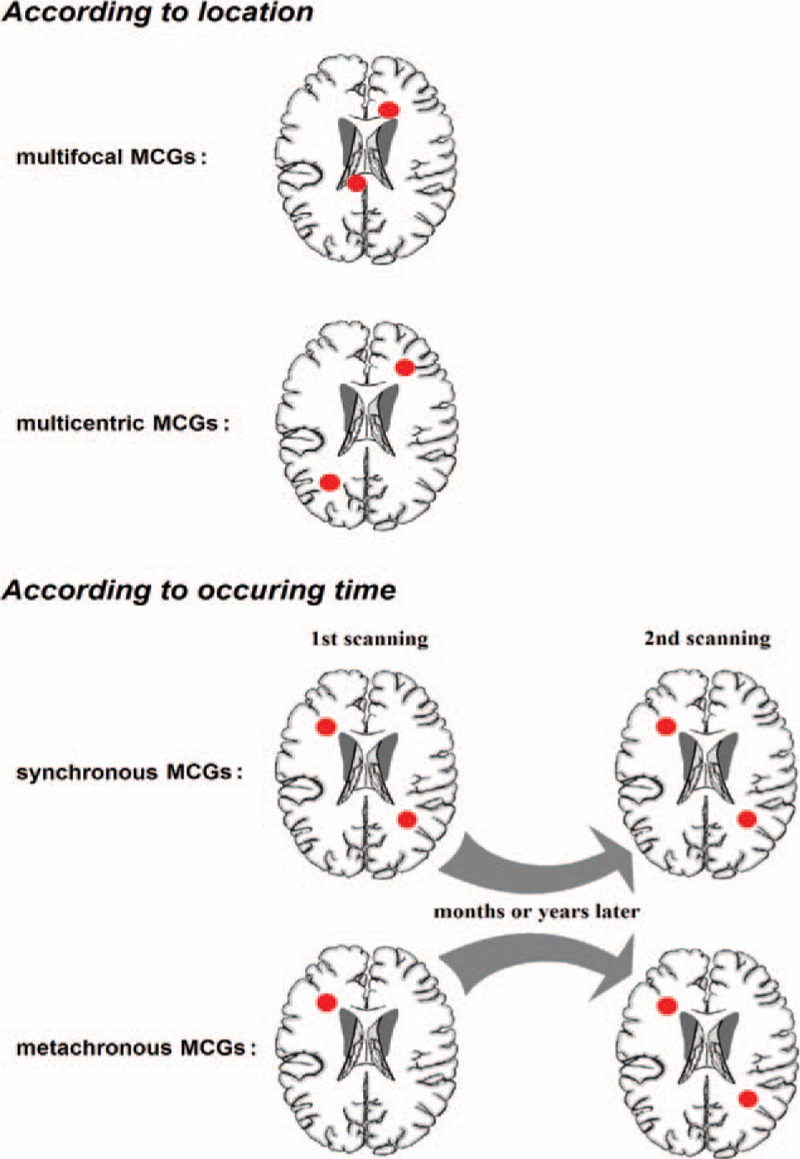
Rationale: Multiple cerebral gliomas (MCGs), usually classified into multifocal and multicentric subtypes, represent major diagnostic challenges as their clinical, radiologic, and pathohistological features are not uniform, often mimicking brain metastatic tumors or central nervous system inflammatory demyelinating diseases (IDD).
Patient concerns: Here, we report a rare case of MCGs with isolated seizures and 4 lesions in the brain, that was initially misdiagnosed as IDD during treatment.
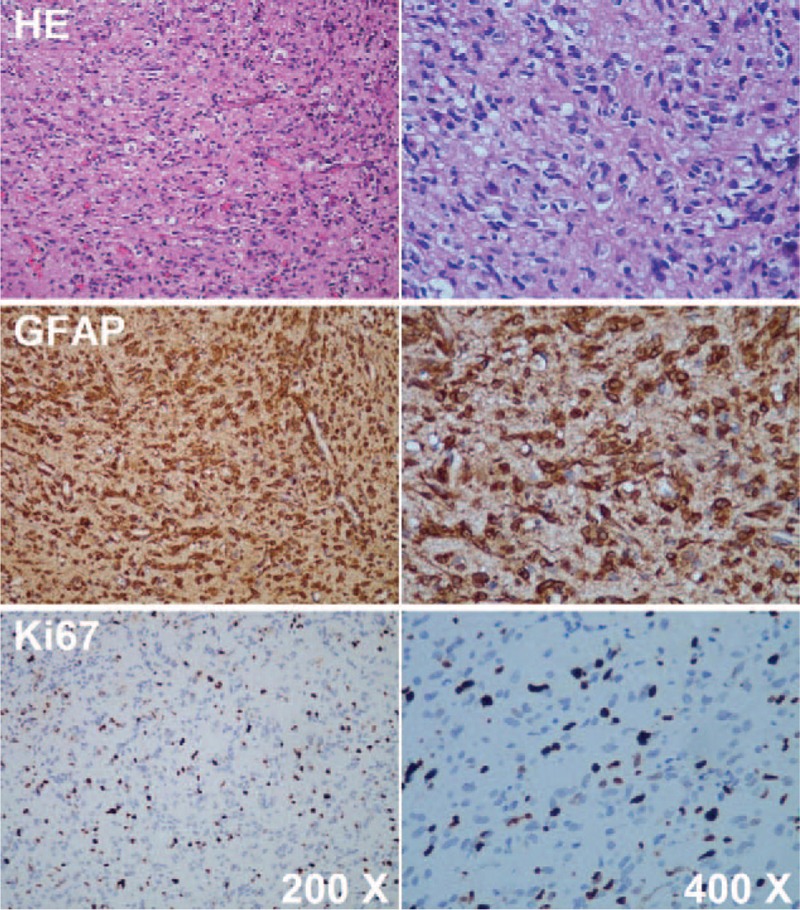
Diagnosis: The pathological diagnosis was astrocytoma, which was classified as a World Health Organization grade II glioma.
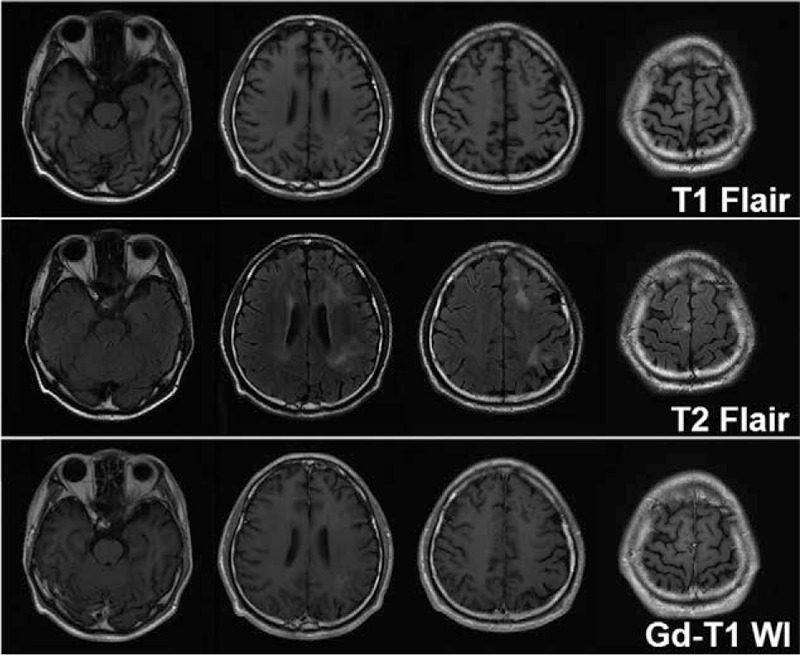
Interventions: The patient was treated with dexamethasone and sodium valproate when he was misdiagnosed as having IDD. After the pathological diagnosis was obtained, he was treated with temozolomide and radiotherapy.
Outcomes: Three months after the above treatment, the health of the patient had improved; he was asymptomatic, and presented with better radiological manifestations.
Lessons: Diagnostic imaging is valuable in differential diagnosis. Magnetic resonance spectroscopy is a promising technique for the assessment and characterization of lesions, though its role in definitive diagnosis is not yet defined. Brain tissue biopsy remains the golden standard for definitive diagnosis. In China, for various reasons, craniotomy biopsy is not performed routinely in patients with multiple intracranial lesions, and stereotactic cranial biopsy may be a more viable option because of its safety and cost-effectiveness. In summary, this case demonstrates that MCGs need to be included in the differential diagnosis of unknown intracranial multiple lesions.
Copyright © 2017 The Authors. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Garcia Pulido P, Neal J, Halpin S, et al. Multicentric oligodendroglioma: case report and review of the literature. Seizure 2013;22:480–2. - PubMed
-
- Salvati M, Caroli E, Orlando ER, et al. Multicentric glioma: our experience in 25 patients and critical review of the literature. Neurosurg Rev 2003;26:275–9. - PubMed
-
- Hyare H, Thust S, Rees J. Advanced MRI techniques in the monitoring of treatment of gliomas. Curr Treat Options Neurol 2017;19:11. - PubMed
-
- Salvati M, Cervoni L, Celli P, et al. Multicentric and multifocal primary cerebral tumours. Methods of diagnosis and treatment. Ital J Neurol Sci 1997;18:17–20. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
