

The dose-response association between estimated glomerular filtration rate and prognosis of patients with ST-segment elevation myocardial infarction from rural areas of China's Liaoning province
- PMID: 29384954
- PMCID: PMC6392960
- DOI: 10.1097/MD.0000000000009508
The dose-response association between estimated glomerular filtration rate and prognosis of patients with ST-segment elevation myocardial infarction from rural areas of China's Liaoning province
Erratum in
-
The dose-response association between estimated glomerular filtration rate and prognosis of patients with ST-segment elevation myocardial infarction from rural areas of China's Liaoning province: Erratum.Medicine (Baltimore). 2018 Mar;97(12):e0259. doi: 10.1097/MD.0000000000010259. Medicine (Baltimore). 2018. PMID: 29561456 Free PMC article. No abstract available.
Abstract
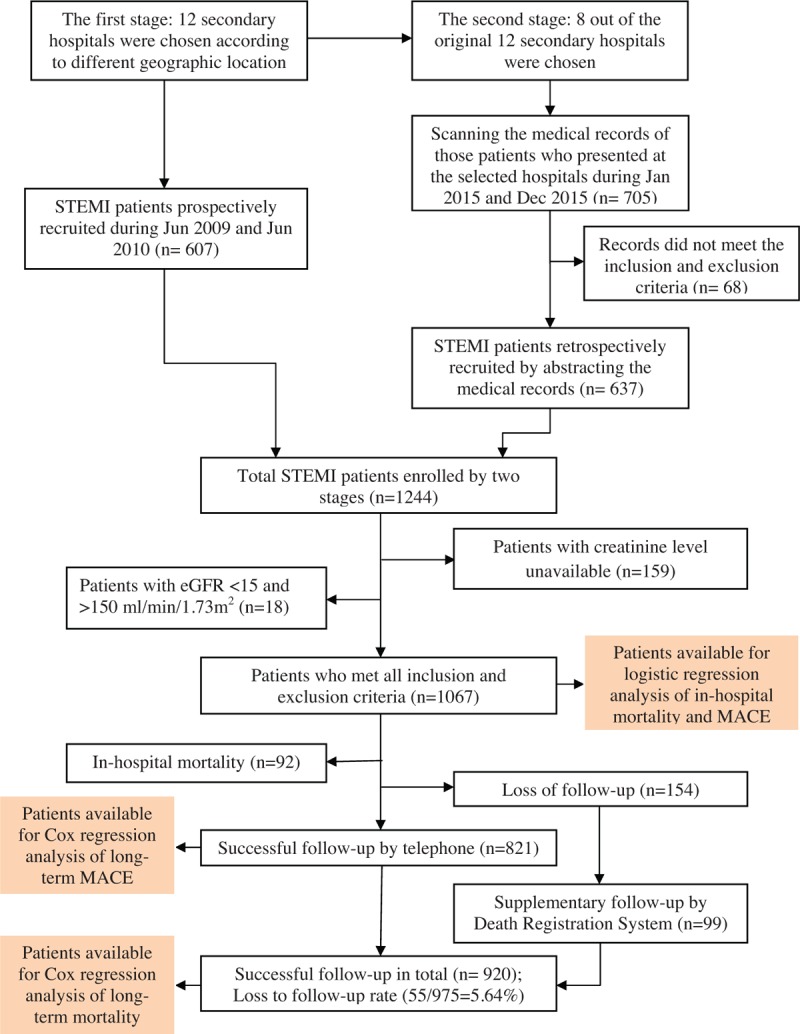
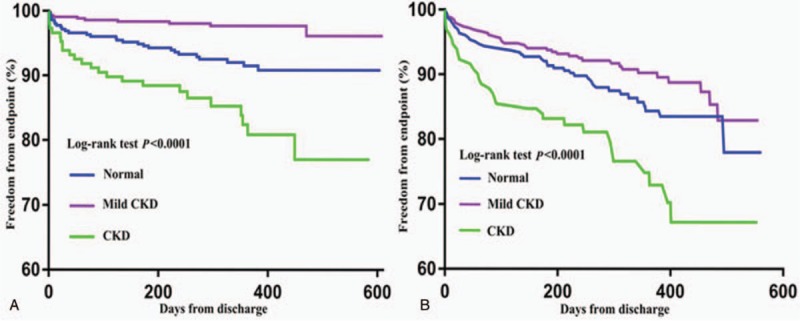
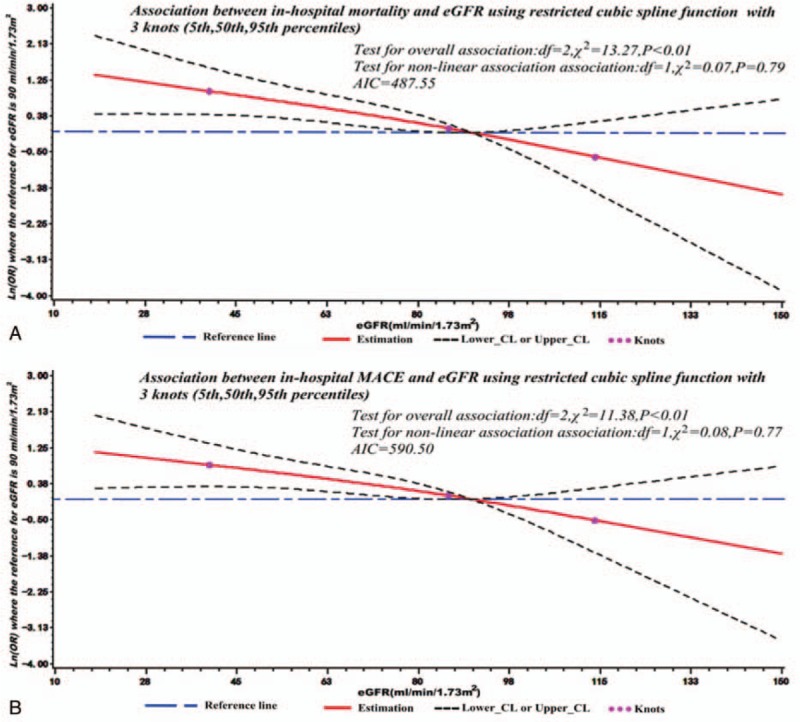
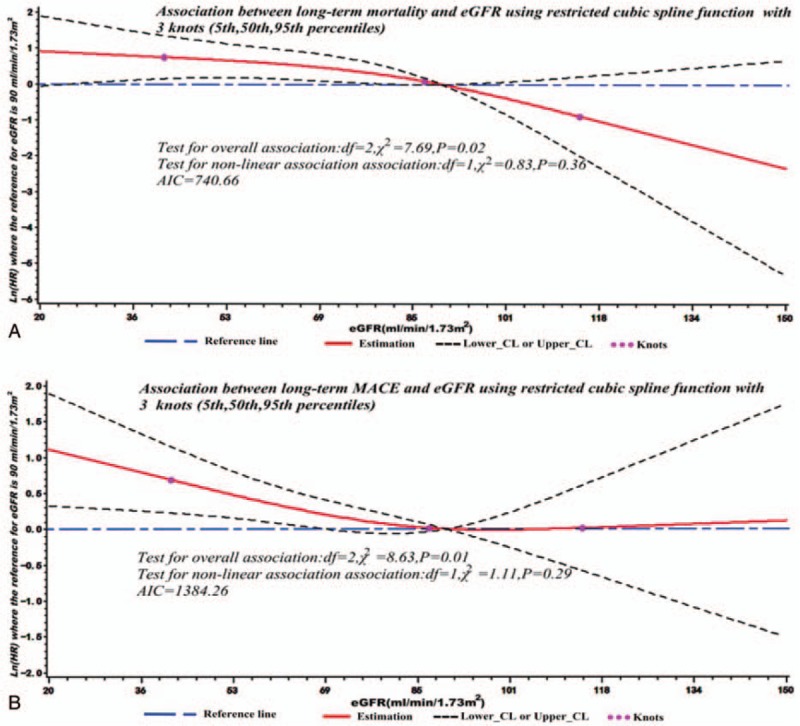
We aimed to investigate the dose-response associations between chronic kidney disease (CKD), and short and long-term cardiovascular outcomes, to characterize these associations by drawing dose-response curves based on a Chinese rural ST-segment elevation myocardial infarction (STEMI) population.In all, 1067 patients with STEMI were consecutively enrolled from 12 secondary hospitals of China's Liaoning province (from June 2009 to June 2010 and January 2015 to December 2015). The follow-up was regularly performed by telephone. Patients were grouped by estimated glomerular filter rate (eGFR): normal, eGFR ≥90 mL/min/1.73 m; mild CKD, 60 to 90 mL/min/1.73 m; CKD, <60 mL/min/1.73 m. Adjusted logistic or Cox regression models were employed to compare short and long-term cardiovascular outcomes across different eGFR groups. Dose-response curves were plotted using restricted cubic spline functions.About 18.46% of the STEMI patients had CKD. Patients with CKD were more likely to suffer from other comorbidities, but less likely to receive evidence-based therapies. CKD was independently associated with in-hospital mortality and major adverse cardiac events (MACE) as compared with patients with normal renal function (for in-hospital mortality, adjusted odds ratio [OR] 2.39, 95% confidence interval [CI] 1.18-4.85, P = .02; for in-hospital MACE, adjusted OR 2.01, 95% CI 1.09-3.70, P < .01). Likewise, CKD was significantly associated with long-term mortality as well (CKD vs normal, adjusted hazard ratio 2.55, 95% CI 1.17-5.57, P = .02). The dose-response associations between eGFR, and short and long-term cardiovascular outcomes were found to be linear (all with P values for nonlinear associations >.05).CKD is an independent predictor of worse in-hospital and long-term clinical outcomes. The assessment of eGFR is essential to enable risk stratification, tailored therapy, and early and aggressive management.
Copyright © 2017 The Authors. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Impact of chronic kidney disease on mortality in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention. A long-term single-center mortality study.Minerva Cardioangiol. 2018 Feb;66(1):6-15. doi: 10.23736/S0026-4725.17.04506-6. Epub 2017 Sep 25. Minerva Cardioangiol. 2018. PMID: 28948753
-
The impact of stage of chronic kidney disease on the outcomes of diabetics with acute myocardial infarction treated with percutaneous coronary intervention.Int Urol Nephrol. 2016 Jul;48(7):1137-43. doi: 10.1007/s11255-016-1260-9. Epub 2016 Mar 19. Int Urol Nephrol. 2016. PMID: 26995007
-
Impact of baseline estimated glomerular filtration rate on inhospital outcomes of patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention: A China acute myocardial infarction registry study.Catheter Cardiovasc Interv. 2019 Feb 15;93(S1):793-799. doi: 10.1002/ccd.28060. Epub 2019 Jan 13. Catheter Cardiovasc Interv. 2019. PMID: 30637931
-
Management and Outcomes of ST-Segment Elevation Myocardial Infarction in US Renal Transplant Recipients.JAMA Cardiol. 2017 Mar 1;2(3):250-258. doi: 10.1001/jamacardio.2016.5131. JAMA Cardiol. 2017. PMID: 28097322
-
Outcomes of STEMI patients with chronic kidney disease treated with percutaneous coronary intervention: the Malaysian National Cardiovascular Disease Database - Percutaneous Coronary Intervention (NCVD-PCI) registry data from 2007 to 2014.BMC Cardiovasc Disord. 2018 Sep 24;18(1):184. doi: 10.1186/s12872-018-0919-9. BMC Cardiovasc Disord. 2018. PMID: 30249197 Free PMC article.
Cited by
-
Dose-response associations between metabolic indexes and the risk of comorbid type 2 diabetes mellitus among rheumatoid arthritis patients from Northern China: a case-control study.BMJ Open. 2019 Jul 4;9(7):e028011. doi: 10.1136/bmjopen-2018-028011. BMJ Open. 2019. PMID: 31278101 Free PMC article.
-
Effect of glomerular filtration rate in patients undergoing percutaneous coronary intervention: A systematic review and meta-analysis.Medicine (Baltimore). 2022 Nov 4;101(44):e31498. doi: 10.1097/MD.0000000000031498. Medicine (Baltimore). 2022. PMID: 36343078 Free PMC article.
-
Prognostic Value of Combining Apelin-12 and Estimated Glomerular Filtration Rate in Patients with ST-Segment Elevation Myocardial Infarction.J Interv Cardiol. 2022 Jun 24;2022:2272928. doi: 10.1155/2022/2272928. eCollection 2022. J Interv Cardiol. 2022. PMID: 35847238 Free PMC article.
-
The dose-response association between estimated glomerular filtration rate and prognosis of patients with ST-segment elevation myocardial infarction from rural areas of China's Liaoning province: Erratum.Medicine (Baltimore). 2018 Mar;97(12):e0259. doi: 10.1097/MD.0000000000010259. Medicine (Baltimore). 2018. PMID: 29561456 Free PMC article. No abstract available.
References
-
- Montalescot G, Dallongeville J, Van Belle E, et al. STEMI and NSTEMI: are they so different? 1 year outcomes in acute myocardial infarction as defined by the ESC/ACC definition (the OPERA registry). Eur Heart J 2007;28:1409–17. - PubMed
-
- Turpie AG. Burden of disease: medical and economic impact of acute coronary syndromes. Am J Manag Care 2006;12:S430–4. - PubMed
-
- Chen WW, Gao RL, Liu LS. Summary of China Cardiovascular Report 2015. Chin Circ J 2016;31:624–32.
-
- Gao R, Patel A, Gao W, et al. Prospective observational study of acute coronary syndromes in China: practice patterns and outcomes. Heart 2008;94:554–60. - PubMed
-
- Chen ZM, Jiang LX, Chen YP, et al. Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet 2005;366:1607–21. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
