

Near-Patient Sampling to Assist Infection Control-A Case Report and Discussion
- PMID: 29385031
- PMCID: PMC5858307
- DOI: 10.3390/ijerph15020238
Near-Patient Sampling to Assist Infection Control-A Case Report and Discussion
Abstract
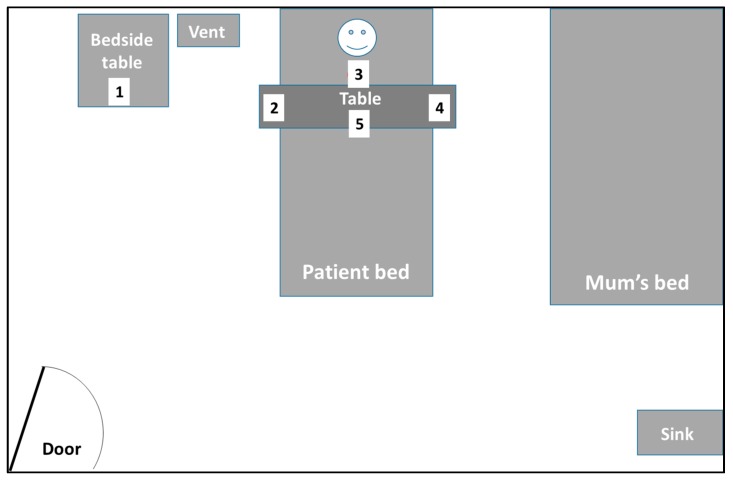
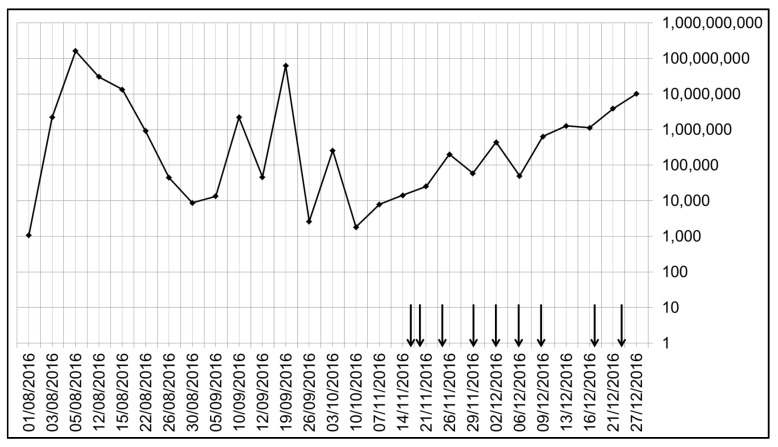
Air sampling as an aid to infection control is still in an experimental stage, as there is no consensus about which air samplers and pathogen detection methods should be used, and what thresholds of specific pathogens in specific exposed populations (staff, patients, or visitors) constitutes a true clinical risk. This case report used a button sampler, worn or held by staff or left free-standing in a fixed location, for environmental sampling around a child who was chronically infected by a respiratory adenovirus, to determine whether there was any risk of secondary adenovirus infection to the staff managing the patient. Despite multiple air samples taken on difference days, coinciding with high levels of adenovirus detectable in the child's nasopharyngeal aspirates (NPAs), none of the air samples contained any detectable adenovirus DNA using a clinically validated diagnostic polymerase chain reaction (PCR) assay. Although highly sensitive, in-house PCR assays have been developed to detect airborne pathogen RNA/DNA, it is still unclear what level of specific pathogen RNA/DNA constitutes a true clinical risk. In this case, the absence of detectable airborne adenovirus DNA using a conventional diagnostic assay removed the requirement for staff to wear surgical masks and face visors when they entered the child's room. No subsequent staff infections or outbreaks of adenovirus have so far been identified.
Keywords: adenovirus; air sampling; airborne; face masks; infection control; limit of detection; personal protective equipment; respiratory; sensitivity; transmission.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Surveillance of airborne adenovirus and Mycoplasma pneumoniae in a hospital pediatric department.PLoS One. 2012;7(3):e33974. doi: 10.1371/journal.pone.0033974. Epub 2012 Mar 21. PLoS One. 2012. PMID: 22470502 Free PMC article.
-
Airborne SARS-CoV-2 in home and hospital environments investigated with a high-powered air sampler.J Hosp Infect. 2022 Jan;119:126-131. doi: 10.1016/j.jhin.2021.10.018. Epub 2021 Nov 6. J Hosp Infect. 2022. PMID: 34752804 Free PMC article.
-
Using a bioaerosol personal sampler in combination with real-time PCR analysis for rapid detection of airborne viruses.Environ Microbiol. 2007 Apr;9(4):992-1000. doi: 10.1111/j.1462-2920.2006.01226.x. Environ Microbiol. 2007. PMID: 17359271
-
Peritonsillar abscess: clinical aspects of microbiology, risk factors, and the association with parapharyngeal abscess.Dan Med J. 2017 Mar;64(3):B5333. Dan Med J. 2017. PMID: 28260599 Review.
-
Methods for sampling of airborne viruses.Microbiol Mol Biol Rev. 2008 Sep;72(3):413-44. doi: 10.1128/MMBR.00002-08. Microbiol Mol Biol Rev. 2008. PMID: 18772283 Free PMC article. Review.
Cited by
-
Comparison of three air samplers for the collection of four nebulized respiratory viruses - Collection of respiratory viruses from air.Indoor Air. 2021 Nov;31(6):1874-1885. doi: 10.1111/ina.12875. Epub 2021 Jun 14. Indoor Air. 2021. PMID: 34124803 Free PMC article.
-
Editorial: the airborne microbiome - implications for aerosol transmission and infection control - special issue.BMC Infect Dis. 2019 Aug 29;19(1):755. doi: 10.1186/s12879-019-4399-z. BMC Infect Dis. 2019. PMID: 31464601 Free PMC article.
-
Airborne Transmission of Influenza Virus in a Hospital of Qinhuangdao During 2017-2018 Flu Season.Food Environ Virol. 2019 Dec;11(4):427-439. doi: 10.1007/s12560-019-09404-1. Epub 2019 Sep 23. Food Environ Virol. 2019. PMID: 31549297
-
Healthcare personnel exposure in an emergency department during influenza season.PLoS One. 2018 Aug 31;13(8):e0203223. doi: 10.1371/journal.pone.0203223. eCollection 2018. PLoS One. 2018. PMID: 30169507 Free PMC article.
-
Influenza virus RNA recovered from droplets and droplet nuclei emitted by adults in an acute care setting.J Occup Environ Hyg. 2019 May;16(5):341-348. doi: 10.1080/15459624.2019.1591626. Epub 2019 May 3. J Occup Environ Hyg. 2019. PMID: 31050610 Free PMC article.
References
-
- Booth T.F., Kournikakis B., Bastien N., Ho J., Kobasa D., Stadnyk L., Li Y., Spence M., Paton S., Henry B., et al. Detection of airborne severe acute respiratory syndrome (SARS) coronavirus and environmental contamination in SARS outbreak units. J. Infect. Dis. 2005;191:1472–1477. doi: 10.1086/429634. - DOI - PMC - PubMed
-
- Matuka O., Singh T.S., Bryce E., Yassi A., Kgasha O., Zungu M., Kyaw K., Malotle M., Renton K., O’Hara L. Pilot study to detect airborne Mycobacterium tuberculosis exposure in a South African public healthcare facility outpatient clinic. J. Hosp. Infect. 2015;89:192–196. doi: 10.1016/j.jhin.2014.11.013. - DOI - PubMed
-
- Lindsley W.G., Blachere F.M., Davis K.A., Pearce T.A., Fisher M.A., Khakoo R., Davis S.M., Rogers M.E., Thewlis R.E., Posada J.A., et al. Distribution of airborne influenza virus and respiratory syncytial virus in an urgent care medical clinic. Clin. Infect. Dis. 2010;50:693–698. doi: 10.1086/650457. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
