

Nabiximols combined with motivational enhancement/cognitive behavioral therapy for the treatment of cannabis dependence: A pilot randomized clinical trial
- PMID: 29385147
- PMCID: PMC5791962
- DOI: 10.1371/journal.pone.0190768
Nabiximols combined with motivational enhancement/cognitive behavioral therapy for the treatment of cannabis dependence: A pilot randomized clinical trial
Abstract
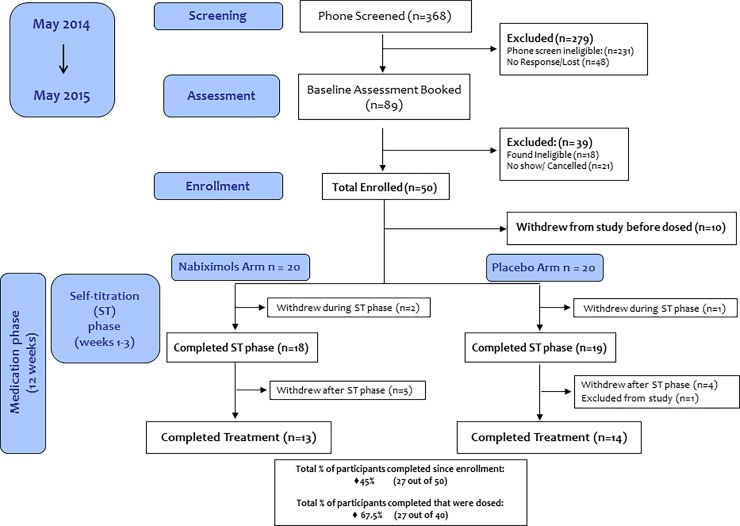
Background: The current lack of pharmacological treatments for cannabis use disorder (CUD) warrants novel approaches and further investigation of promising pharmacotherapy. We previously showed that nabiximols (27 mg/ml Δ9-tetrahydrocannabinol (THC)/ 25 mg/ml cannabidiol (CBD), Sativex®) can decrease cannabis withdrawal symptoms. Here, we assessed in a pilot study the tolerability and safety of self-titrated nabiximols vs. placebo among 40 treatment-seeking cannabis-dependent participants.
Methods: Subjects participated in a double blind randomized clinical trial, with as-needed nabiximols up to 113.4 mg THC/105 mg CBD or placebo daily for 12 weeks, concurrently with Motivational Enhancement Therapy and Cognitive Behavioral Therapy (MET/CBT). Primary outcome measures were tolerability and abstinence, secondary outcome measures were days and amount of cannabis use, withdrawal, and craving scores. Participants received up to CDN$ 855 in compensation for their time.
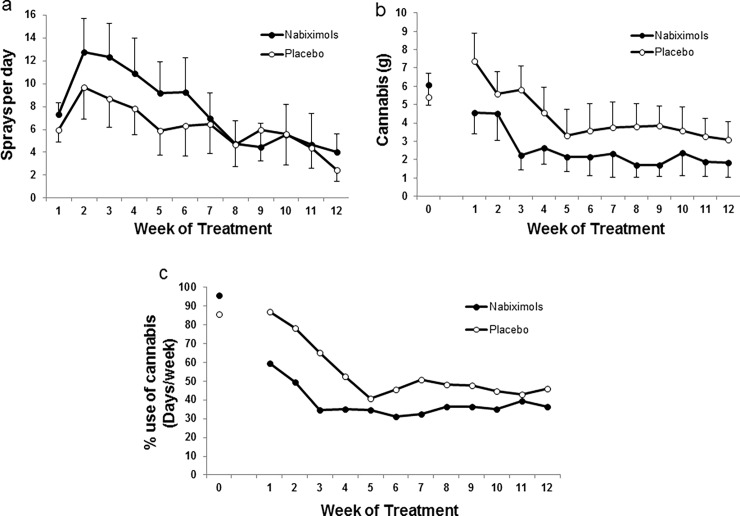
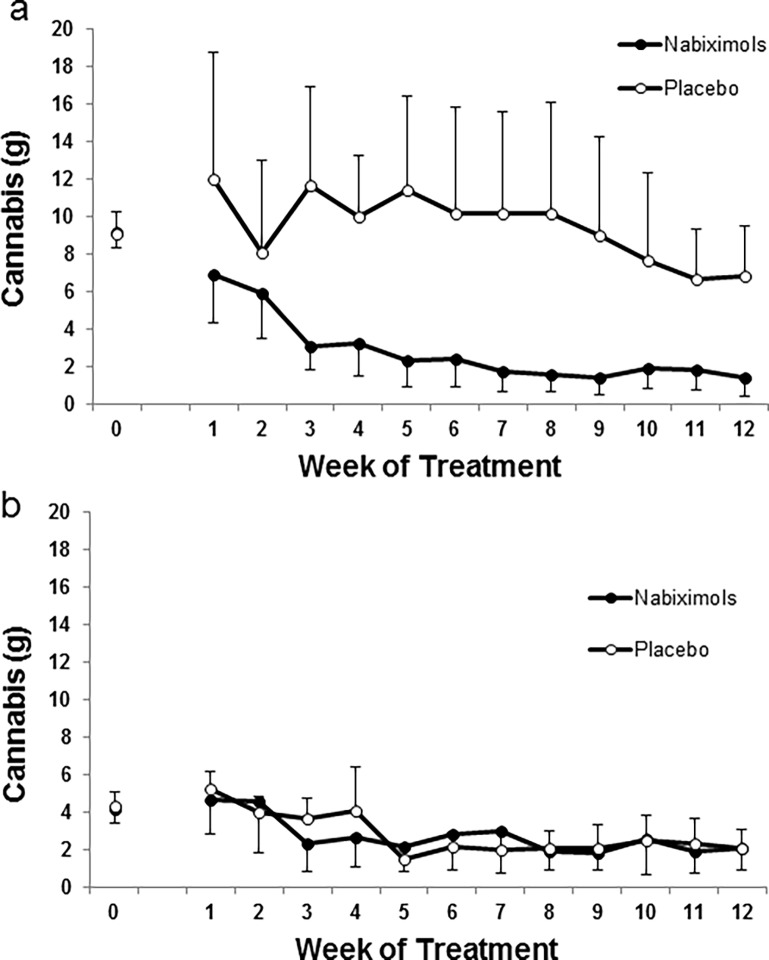
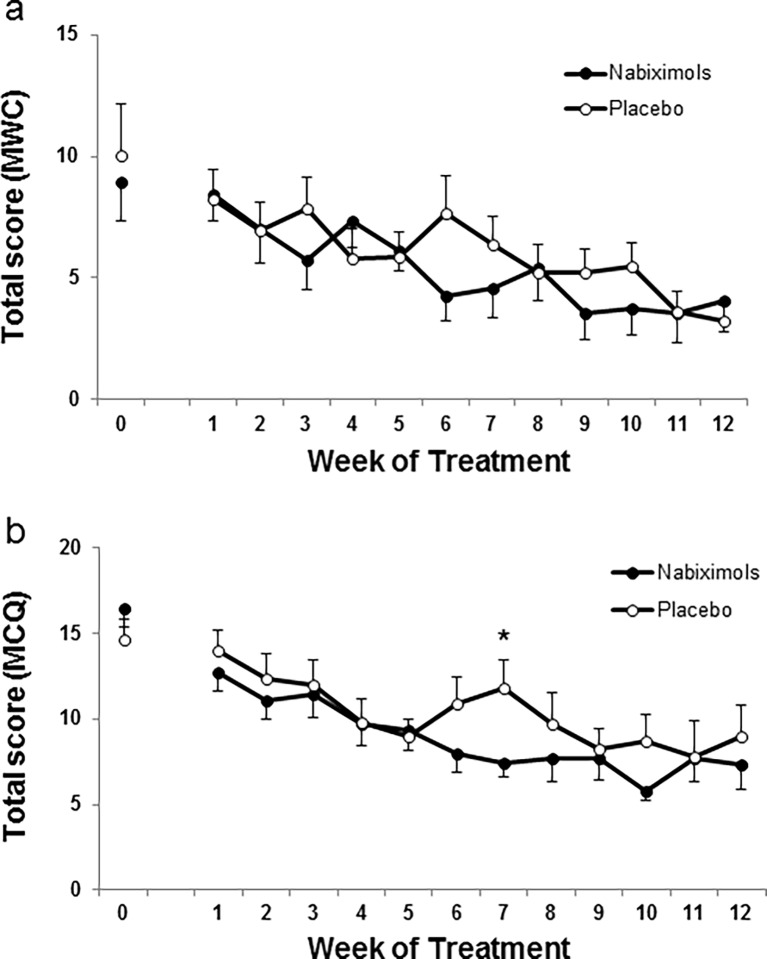
Results: Medication was well tolerated and no serious adverse events (SAEs) were observed. Rates of adverse events did not differ between treatment arms (F1,39 = 0.205, NS). There was no significant change in abstinence rates at trial end. Participants were not able to differentiate between subjective effects associated with nabiximols or placebo treatments (F1,40 = 0.585, NS). Cannabis use was reduced in the nabiximols (70.5%) and placebo groups (42.6%). Nabiximols reduced cannabis craving but no significant differences between the nabiximols and placebo groups were observed on withdrawal scores.
Conclusions: Nabiximols in combination with MET/CBT was well tolerated and allowed for reduction of cannabis use. Future clinical trials should explore the potential of high doses of nabiximols for cannabis dependence.
Conflict of interest statement
Figures
References
-
- UNODC (2016) United Nations Office on Drugs and Crime. World Drug Report 2016. New York: United Nations.
-
- UNODC (2015) United Nations Office on Drugs and Crime. World Drug Report 2015. In: Nations U, editor. New York
-
- Room R, Fischer B, Hall W, Lenton S, Reuter P, editors (2010) Cannabis policy: Moving beyond stalemate. New York, NY: Oxford University Press.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
