

Improvements in bladder, bowel and sexual outcomes following task-specific locomotor training in human spinal cord injury
- PMID: 29385166
- PMCID: PMC5791974
- DOI: 10.1371/journal.pone.0190998
Improvements in bladder, bowel and sexual outcomes following task-specific locomotor training in human spinal cord injury
Abstract
Objective: Locomotor training (LT) as a therapeutic intervention following spinal cord injury (SCI) is an effective rehabilitation strategy for improving motor outcomes, but its impact on non-locomotor functions is unknown. Given recent results of our labs' pre-clinical animal SCI LT studies and existing overlap of lumbosacral spinal circuitries controlling pelvic-visceral and locomotor functions, we addressed whether LT can improve bladder, bowel and sexual function in humans at chronic SCI time-points (> two years post-injury).
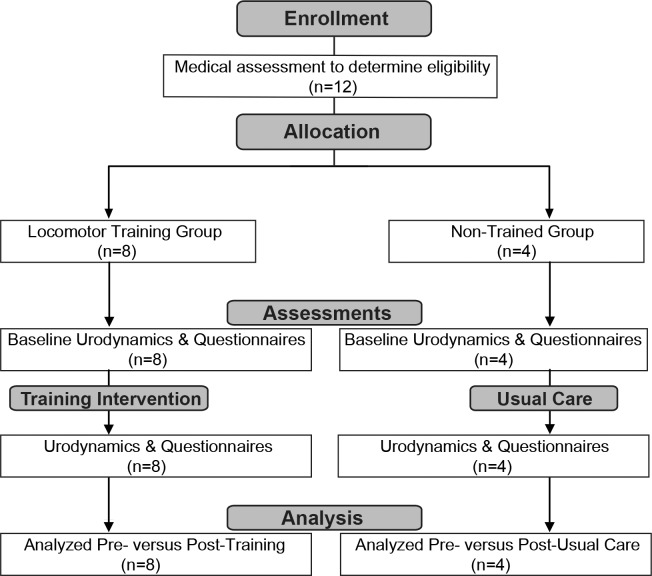
Study design: Prospective cohort study; pilot trial with small sample size.
Methods: Eight SCI research participants who were undergoing 80 daily one-hour sessions of LT on a treadmill using body-weight support, or one-hour of LT and stand training on alternate days, as part of another research study conducted at the Kentucky Spinal Cord Injury Research Center, University of Louisville, were enrolled in this pilot trial. Urodynamic assessments were performed and International Data Set questionnaire forms completed for bladder, bowel and sexual functions at pre-and post-training time points. Four usual care (non-trained; regular at-home routine) research participants were also enrolled in this study and had the same assessments collected twice, at least 3 months apart.
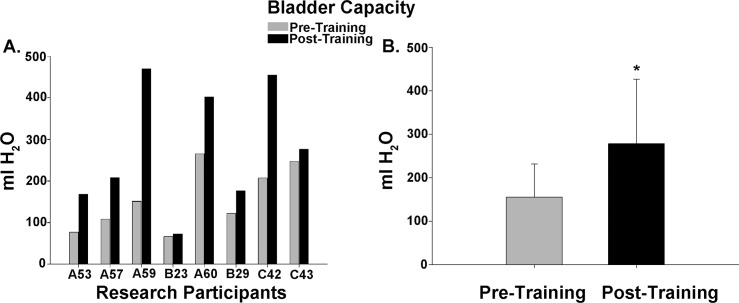
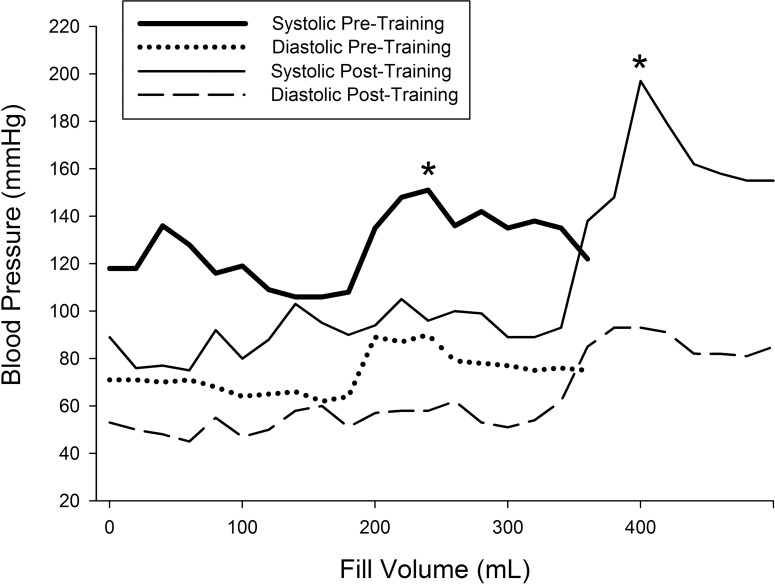
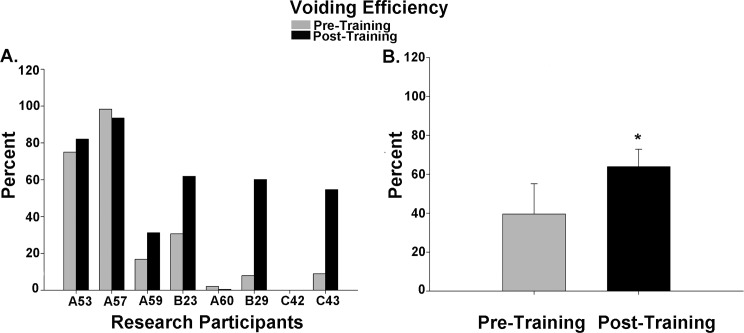
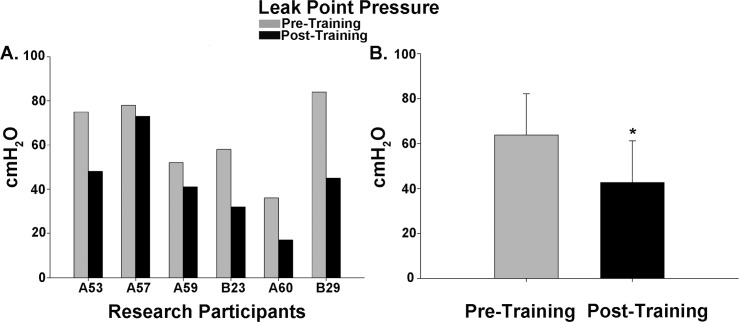
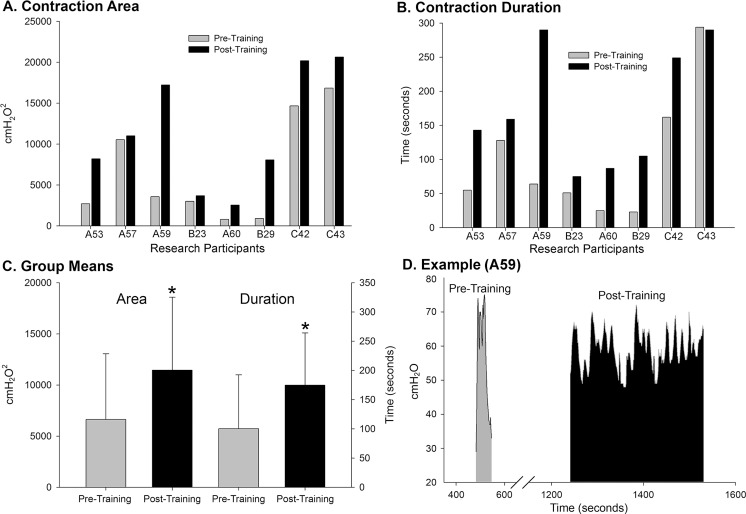
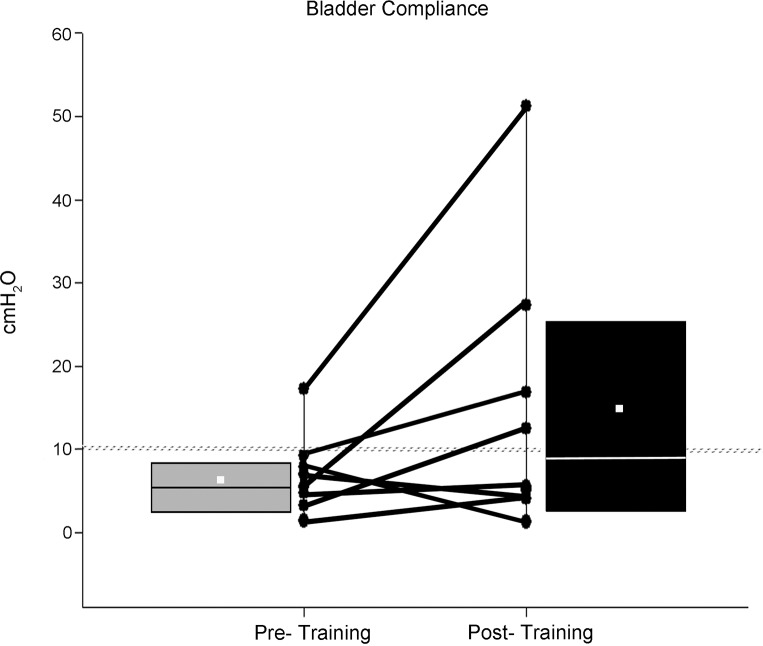
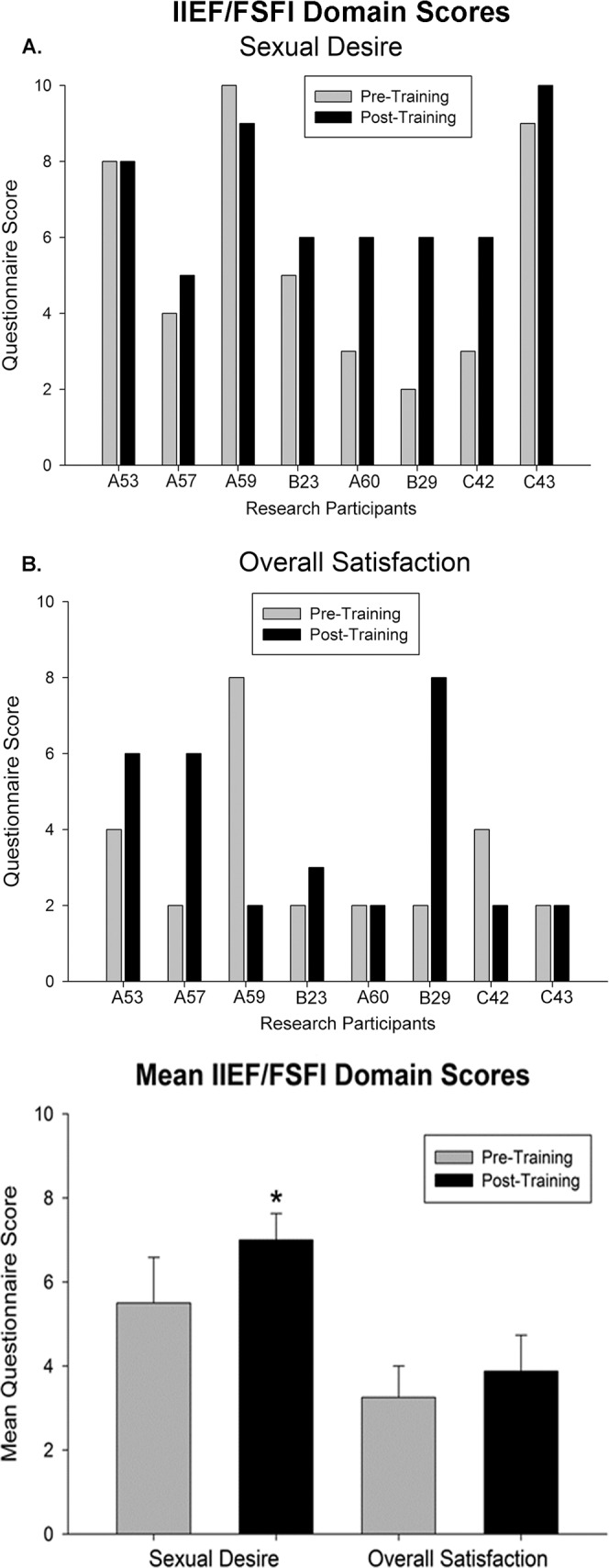
Results: Filling cystometry documented significant increases in bladder capacity, voiding efficiency and detrusor contraction time as well as significant decreases in voiding pressure post-training relative to baseline. Questionnaires revealed a decrease in the frequency of nocturia and urinary incontinence for several research participants as well as a significant decrease in time required for defecation and a significant increase in sexual desire post-training. No significant differences were found for usual care research participants.
Conclusions: These results suggest that an appropriate level of sensory information provided to the spinal cord, generated through task-specific stepping and/or loading, can positively benefit the neural circuitries controlling urogenital and bowel functions.
Trial registration: ClinicalTrials.gov NCT03036527.
Conflict of interest statement
Figures



References
-
- Anderson KD. Targeting recovery: priorities of the spinal cord-injured population. J Neurotrauma. 2004;21(10):1371–83. doi: 10.1089/neu.2004.21.1371 - DOI - PubMed
-
- Ditunno PL, Patrick M, Stineman M, Ditunno JF. Who wants to walk? Preferences for recovery after SCI: a longitudinal and cross-sectional study. Spinal Cord. 2008;46(7):500–6. doi: 10.1038/sj.sc.3102172 - DOI - PubMed
-
- Han TR, Kim JH, Kwon BS. Chronic gastrointestinal problems and bowel dysfunction in patients with spinal cord injury. Spinal Cord. 1998;36(7):485–90. - PubMed
-
- Groen J, Pannek J, Castro Diaz D, Del Popolo G, Gross T, Hamid R, et al. Summary of European Association of Urology (EAU) Guidelines on Neuro-Urology. Eur Urol. 2016;69(2):324–33. doi: 10.1016/j.eururo.2015.07.071 - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
