

Sexual Dimorphism and the Origins of Human Spinal Health
- PMID: 29385433
- PMCID: PMC5888211
- DOI: 10.1210/er.2017-00147
Sexual Dimorphism and the Origins of Human Spinal Health
Abstract
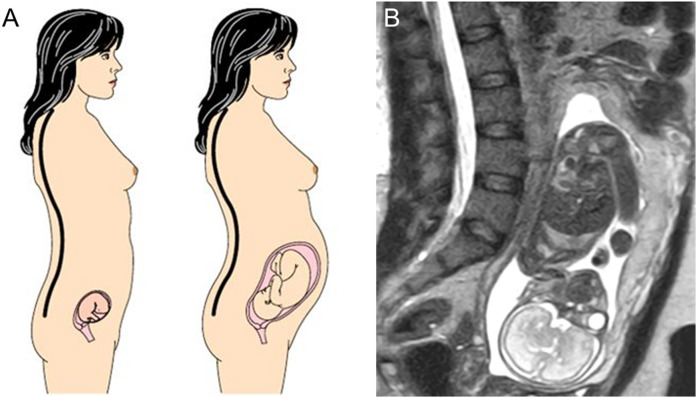
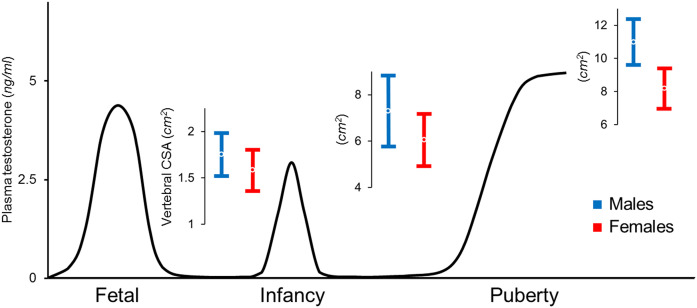
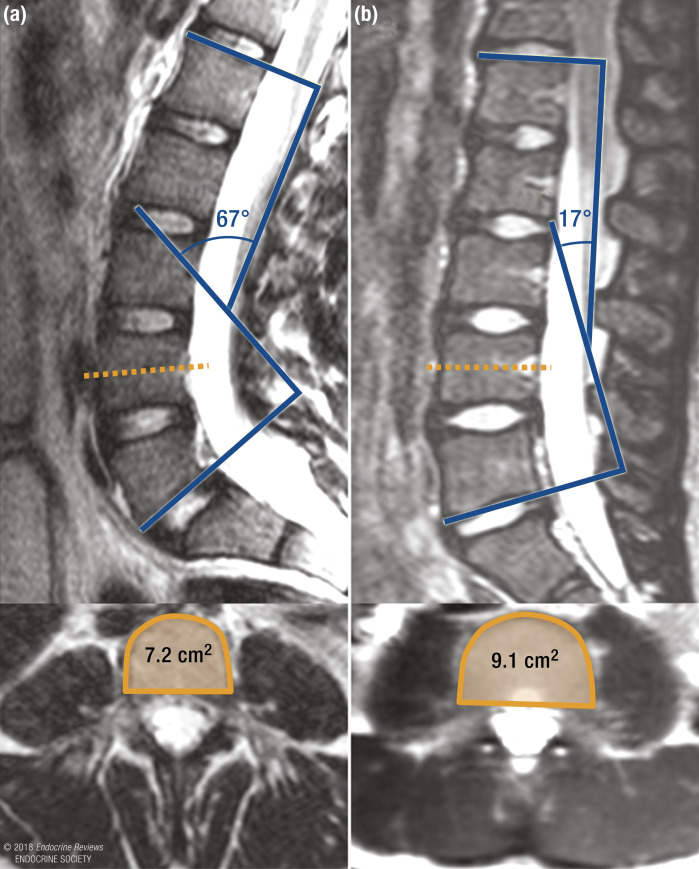
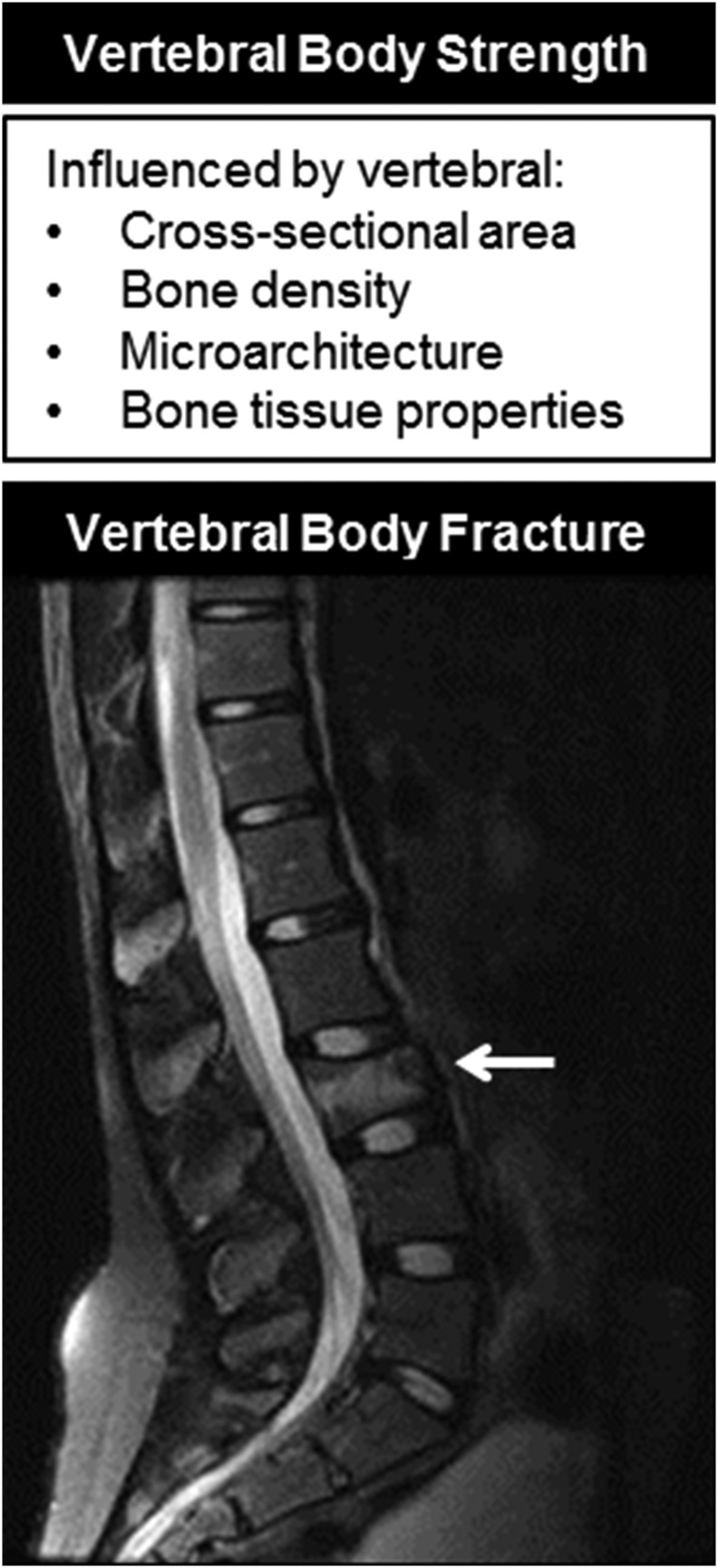
Recent observations indicate that the cross-sectional area (CSA) of vertebral bodies is on average 10% smaller in healthy newborn girls than in newborn boys, a striking difference that increases during infancy and puberty and is greatest by the time of sexual and skeletal maturity. The smaller CSA of female vertebrae is associated with greater spinal flexibility and could represent the human adaptation to fetal load in bipedal posture. Unfortunately, it also imparts a mechanical disadvantage that increases stress within the vertebrae for all physical activities. This review summarizes the potential endocrine, genetic, and environmental determinants of vertebral cross-sectional growth and current knowledge of the association between the small female vertebrae and greater risk for a broad array of spinal conditions across the lifespan.
Figures
References
-
- Antoniades L, MacGregor AJ, Andrew T, Spector TD. Association of birth weight with osteoporosis and osteoarthritis in adult twins. Rheumatology (Oxford). 2003;42(6):791–796. - PubMed
-
- Dennison EM, Syddall HE, Sayer AA, Gilbody HJ, Cooper C. Birth weight and weight at 1 year are independent determinants of bone mass in the seventh decade: the Hertfordshire cohort study. Pediatr Res. 2005;57(4):582–586. - PubMed
-
- Cooper C, Westlake S, Harvey N, Javaid K, Dennison E, Hanson M. Review: developmental origins of osteoporotic fracture. Osteoporos Int. 2006;17(3):337–347. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
