

Variation of poorly ventilated lung units (silent spaces) measured by electrical impedance tomography to dynamically assess recruitment
- PMID: 29386048
- PMCID: PMC5793388
- DOI: 10.1186/s13054-017-1931-7
Variation of poorly ventilated lung units (silent spaces) measured by electrical impedance tomography to dynamically assess recruitment
Abstract
Background: Assessing alveolar recruitment at different positive end-expiratory pressure (PEEP) levels is a major clinical and research interest because protective ventilation implies opening the lung without inducing overdistention. The pressure-volume (P-V) curve is a validated method of assessing recruitment but reflects global characteristics, and changes at the regional level may remain undetected. The aim of the present study was to compare, in intubated patients with acute hypoxemic respiratory failure (AHRF) and acute respiratory distress syndrome (ARDS), lung recruitment measured by P-V curve analysis, with dynamic changes in poorly ventilated units of the dorsal lung (dependent silent spaces [DSSs]) assessed by electrical impedance tomography (EIT). We hypothesized that DSSs might represent a dynamic bedside measure of recruitment.
Methods: We carried out a prospective interventional study of 14 patients with AHRF and ARDS admitted to the intensive care unit undergoing mechanical ventilation. Each patient underwent an incremental/decremental PEEP trial that included five consecutive phases: PEEP 5 and 10 cmH2O, recruitment maneuver + PEEP 15 cmH2O, then PEEP 10 and 5 cmH2O again. We measured, at the end of each phase, recruitment from previous PEEP using the P-V curve method, and changes in DSS were continuously monitored by EIT.
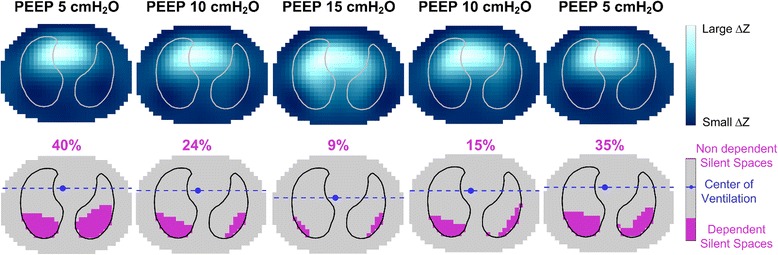
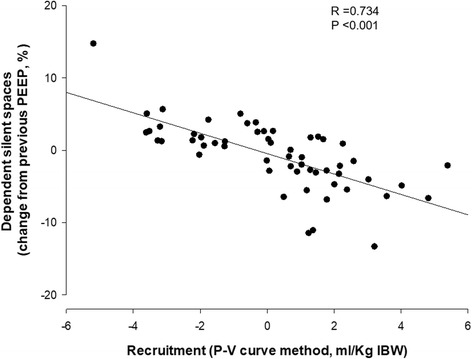
Results: PEEP changes induced alveolar recruitment as assessed by the P-V curve method and changes in the amount of DSS (p < 0.001). Recruited volume measured by the P-V curves significantly correlated with the change in DSS (rs = 0.734, p < 0.001). Regional compliance of the dependent lung increased significantly with rising PEEP (median PEEP 5 cmH2O = 11.9 [IQR 10.4-16.7] ml/cmH2O, PEEP 15 cmH2O = 19.1 [14.2-21.3] ml/cmH2O; p < 0.001), whereas regional compliance of the nondependent lung decreased from PEEP 5 cmH2O to PEEP 15 cmH2O (PEEP 5 cmH2O = 25.3 [21.3-30.4] ml/cmH2O, PEEP 15 cmH2O = 20.0 [16.6-22.8] ml/cmH2O; p <0.001). By increasing the PEEP level, the center of ventilation moved toward the dependent lung, returning to the nondependent lung during the decremental PEEP steps.
Conclusions: The variation of DSSs dynamically measured by EIT correlates well with lung recruitment measured using the P-V curve technique. EIT might provide useful information to titrate personalized PEEP.
Trial registration: ClinicalTrials.gov, NCT02907840 . Registered on 20 September 2016.
Keywords: Acute respiratory distress syndrome; Acute respiratory failure; Electrical impedance tomography; Personalized medicine; Positive end-expiratory pressure; Pressure-volume curve.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the ethics committee of the Sant’Anna Hospital, Ferrara, Italy (protocol no. 141285), and registered with ClinicalTrials.gov (NCT02907840).
Consent for publication
Written informed consent was obtained from the patients or their relatives for publication of their individual details. The consent forms are held by the authors and are available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Heterogeneity of regional inflection points from pressure-volume curves assessed by electrical impedance tomography.Crit Care. 2019 Apr 16;23(1):119. doi: 10.1186/s13054-019-2417-6. Crit Care. 2019. PMID: 30992054 Free PMC article.
-
Assessment of electrical impedance tomography to set optimal positive end-expiratory pressure for veno-venous ECMO-treated severe ARDS patients.J Crit Care. 2020 Dec;60:38-44. doi: 10.1016/j.jcrc.2020.06.017. Epub 2020 Jul 8. J Crit Care. 2020. PMID: 32736198
-
Electrical impedance tomography: A compass for the safe route to optimal PEEP.Respir Med. 2021 Oct;187:106555. doi: 10.1016/j.rmed.2021.106555. Epub 2021 Jul 30. Respir Med. 2021. PMID: 34352563 Review.
-
Bedside Contribution of Electrical Impedance Tomography to Setting Positive End-Expiratory Pressure for Extracorporeal Membrane Oxygenation-treated Patients with Severe Acute Respiratory Distress Syndrome.Am J Respir Crit Care Med. 2017 Aug 15;196(4):447-457. doi: 10.1164/rccm.201605-1055OC. Am J Respir Crit Care Med. 2017. PMID: 28103448
-
Titration of extra-PEEP against intrinsic-PEEP in severe asthma by electrical impedance tomography: A case report and literature review.Medicine (Baltimore). 2020 Jun 26;99(26):e20891. doi: 10.1097/MD.0000000000020891. Medicine (Baltimore). 2020. PMID: 32590795 Free PMC article. Review.
Cited by
-
Prone Positioning Decreases Inhomogeneity and Improves Dorsal Compliance in Invasively Ventilated Spontaneously Breathing COVID-19 Patients-A Study Using Electrical Impedance Tomography.Diagnostics (Basel). 2022 Sep 21;12(10):2281. doi: 10.3390/diagnostics12102281. Diagnostics (Basel). 2022. PMID: 36291970 Free PMC article.
-
Roles of electrical impedance tomography in lung transplantation.Front Physiol. 2022 Nov 3;13:986422. doi: 10.3389/fphys.2022.986422. eCollection 2022. Front Physiol. 2022. PMID: 36407002 Free PMC article. Review.
-
Heterogeneity of regional inflection points from pressure-volume curves assessed by electrical impedance tomography.Crit Care. 2019 Apr 16;23(1):119. doi: 10.1186/s13054-019-2417-6. Crit Care. 2019. PMID: 30992054 Free PMC article.
-
Personalized ventilatory strategy based on lung recruitablity in COVID-19-associated acute respiratory distress syndrome: a prospective clinical study.Crit Care. 2023 Apr 19;27(1):152. doi: 10.1186/s13054-023-04360-6. Crit Care. 2023. PMID: 37076900 Free PMC article.
-
Electrical impedance tomography monitoring in adult ICU patients: state-of-the-art, recommendations for standardized acquisition, processing, and clinical use, and future directions.Crit Care. 2024 Nov 19;28(1):377. doi: 10.1186/s13054-024-05173-x. Crit Care. 2024. PMID: 39563476 Free PMC article. Review.
References
-
- ARDS Definition Task Force Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307:2526–33. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
