

Activity of pembrolizumab in relapsed/refractory NK/T-cell lymphoma
- PMID: 29386072
- PMCID: PMC5793390
- DOI: 10.1186/s13045-018-0559-7
Activity of pembrolizumab in relapsed/refractory NK/T-cell lymphoma
Abstract
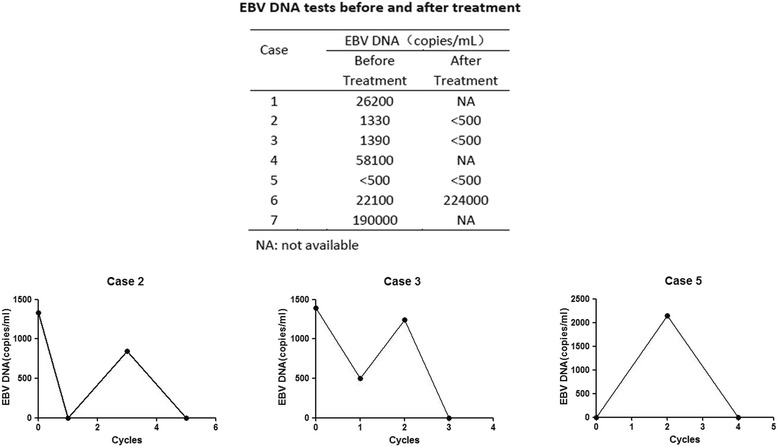
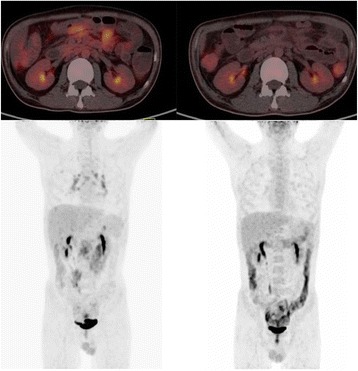
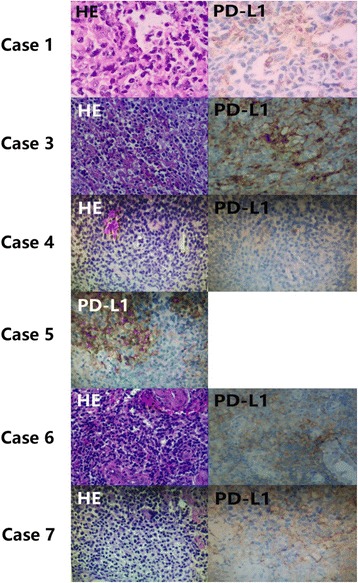
Natural killer/T-cell lymphoma (NKTCL) is a rare subtype of non-Hodgkin lymphoma that is associated with a poor outcome. Currently, the treatment needs of NKTCL remain unmet, and efforts to further improve treatment are urgently needed. Herein, seven patients with NKTCL who failed to respond to various types of chemotherapies were treated with the anti-programmed death 1 (anti-PD-1) antibody pembrolizumab at 100 mg every 3 weeks. After a median of four cycles of treatment (range 2-18), four out of seven patients responded (two complete response, two partial response, overall response rate 57%). Expression of PD1-ligand available was 50, 20, 30, 70, and 30% of five patients respectively. It is negative in one patient and not tested in one patient. Adverse events, which mostly ranged from grade I to grade III, were tolerable and could be safely handled, although immune-related pneumonitis was notable. Overall, PD-1 blockade with pembrolizumab represents a favorable strategy for the treatment of refractory/relapsed NKTCL.
Keywords: NK/T-cell lymphoma; PD-1 blockade; Pembrolizumab.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Zhengzhou University First Affiliated Hospital. All patients provided informed consent.
Consent for publication
Written informed consent for publication was obtained.
Competing interests
The authors declare no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Successful treatment with anti-programmed-death-1 antibody in a relapsed natural killer/T-cell lymphoma patient with multi-line resistance: a case report.BMC Cancer. 2017 Jul 28;17(1):507. doi: 10.1186/s12885-017-3501-4. BMC Cancer. 2017. PMID: 28754096 Free PMC article.
-
Comparison of Efficacy of Pembrolizumab between Epstein-Barr Virus‒Positive and ‒Negative Relapsed or Refractory Non-Hodgkin Lymphomas.Cancer Res Treat. 2019 Apr;51(2):611-622. doi: 10.4143/crt.2018.191. Epub 2018 Jul 20. Cancer Res Treat. 2019. PMID: 30025443 Free PMC article.
-
Phase II Study of the PD-1 Inhibitor Pembrolizumab for the Treatment of Relapsed or Refractory Mature T-cell Lymphoma.Clin Lymphoma Myeloma Leuk. 2019 Jun;19(6):356-364.e3. doi: 10.1016/j.clml.2019.03.022. Epub 2019 Apr 3. Clin Lymphoma Myeloma Leuk. 2019. PMID: 31029646 Free PMC article. Clinical Trial.
-
Updating targets for natural killer/T-cell lymphoma immunotherapy.Cancer Biol Med. 2021 Feb 15;18(1):52-62. doi: 10.20892/j.issn.2095-3941.2020.0400. Cancer Biol Med. 2021. PMID: 33628584 Free PMC article. Review.
-
L’arrivée de l’immunothérapie dans le lymphome de Hodgkin.Bull Cancer. 2018 Dec;105 Suppl 1:S50-S58. doi: 10.1016/S0007-4551(18)30390-4. Bull Cancer. 2018. PMID: 30595199 Review. French.
Cited by
-
Cyclin-dependent kinase 9 as a potential specific molecular target in NK-cell leukemia/lymphoma.Haematologica. 2018 Dec;103(12):2059-2068. doi: 10.3324/haematol.2018.191395. Epub 2018 Aug 3. Haematologica. 2018. PMID: 30076184 Free PMC article.
-
Combination of atezolizumab and chidamide to maintain long-term remission in refractory metastatic extranodal natural killer/T-cell lymphoma: A case report.World J Clin Cases. 2022 Feb 16;10(5):1609-1616. doi: 10.12998/wjcc.v10.i5.1609. World J Clin Cases. 2022. PMID: 35211600 Free PMC article.
-
How we treat NK/T-cell lymphomas.J Hematol Oncol. 2022 Jun 3;15(1):74. doi: 10.1186/s13045-022-01293-5. J Hematol Oncol. 2022. PMID: 35659326 Free PMC article. Review.
-
Towards Next Generation Biomarkers in Natural Killer/T-Cell Lymphoma.Life (Basel). 2021 Aug 16;11(8):838. doi: 10.3390/life11080838. Life (Basel). 2021. PMID: 34440582 Free PMC article. Review.
-
Clinical significance of circulating exosomal PD-L1 and soluble PD-L1 in extranodal NK/T-cell lymphoma, nasal-type.Am J Cancer Res. 2020 Dec 1;10(12):4498-4512. eCollection 2020. Am J Cancer Res. 2020. PMID: 33415014 Free PMC article.
References
-
- Hodi FS, O'Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel JC, Akerley W, van den Eertwegh AJ, Lutzky J, Lorigan P, Vaubel JM, Linette GP, Hogg D, Ottensmeier CH, Lebbe C, Peschel C, Quirt I, Clark JI, Wolchok JD, Weber JS, Tian J, Yellin MJ, Nichol GM, Hoos A, Urba WJ. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363(8):711–723. doi: 10.1056/NEJMoa1003466. - DOI - PMC - PubMed
-
- Robert C, Thomas L, Bondarenko I, O'Day S, Weber J, Garbe C, Lebbe C, Baurain JF, Testori A, Grob JJ, Davidson N, Richards J, Maio M, Hauschild A, Miller WH, Jr, Gascon P, Lotem M, Harmankaya K, Ibrahim R, Francis S, Chen TT, Humphrey R, Hoos A, Wolchok JD. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med. 2011;364(26):2517–2526. doi: 10.1056/NEJMoa1104621. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
