

Migraine and risk of cardiovascular diseases: Danish population based matched cohort study
- PMID: 29386181
- PMCID: PMC5791041
- DOI: 10.1136/bmj.k96
Migraine and risk of cardiovascular diseases: Danish population based matched cohort study
Abstract
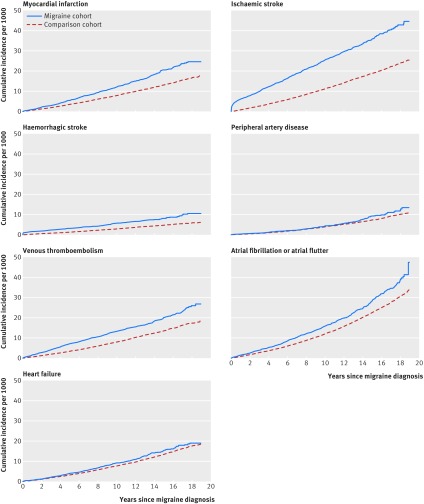
Objective: To examine the risks of myocardial infarction, stroke (ischaemic and haemorrhagic), peripheral artery disease, venous thromboembolism, atrial fibrillation or atrial flutter, and heart failure in patients with migraine and in a general population comparison cohort.
Design: Nationwide, population based cohort study.
Setting: All Danish hospitals and hospital outpatient clinics from 1995 to 2013.
Participants: 51 032 patients with migraine and 510 320 people from the general population matched on age, sex, and calendar year.
Main outcome measures: Comorbidity adjusted hazard ratios of cardiovascular outcomes based on Cox regression analysis.
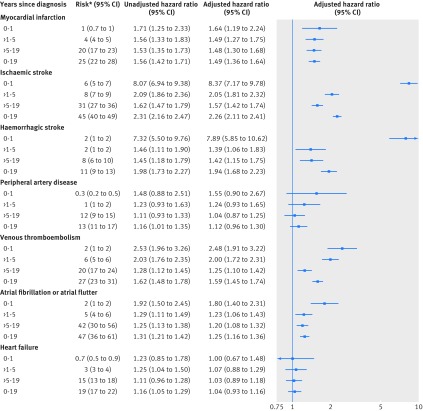
Results: Higher absolute risks were observed among patients with incident migraine than in the general population across most outcomes and follow-up periods. After 19 years of follow-up, the cumulative incidences per 1000 people for the migraine cohort compared with the general population were 25 v 17 for myocardial infarction, 45 v 25 for ischaemic stroke, 11 v 6 for haemorrhagic stroke, 13 v 11 for peripheral artery disease, 27 v 18 for venous thromboembolism, 47 v 34 for atrial fibrillation or atrial flutter, and 19 v 18 for heart failure. Correspondingly, migraine was positively associated with myocardial infarction (adjusted hazard ratio 1.49, 95% confidence interval 1.36 to 1.64), ischaemic stroke (2.26, 2.11 to 2.41), and haemorrhagic stroke (1.94, 1.68 to 2.23), as well as venous thromboembolism (1.59, 1.45 to 1.74) and atrial fibrillation or atrial flutter (1.25, 1.16 to 1.36). No meaningful association was found with peripheral artery disease (adjusted hazard ratio 1.12, 0.96 to 1.30) or heart failure (1.04, 0.93 to 1.16). The associations, particularly for stroke outcomes, were stronger during the short term (0-1 years) after diagnosis than the long term (up to 19 years), in patients with aura than in those without aura, and in women than in men. In a subcohort of patients, the associations persisted after additional multivariable adjustment for body mass index and smoking.
Conclusions: Migraine was associated with increased risks of myocardial infarction, ischaemic stroke, haemorrhagic stroke, venous thromboembolism, and atrial fibrillation or atrial flutter. Migraine may be an important risk factor for most cardiovascular diseases.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organisation for the submitted work other than that detailed above; no financial relationships in the previous three years with any organisations that might have an interest in the submitted work; and no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Migraine and risk of cardiovascular disease.BMJ. 2018 Jan 31;360:k275. doi: 10.1136/bmj.k275. BMJ. 2018. PMID: 29386182 No abstract available.
-
Migraine: Migraine - a risk factor for cardiovascular disease?Nat Rev Neurol. 2018 Apr;14(4):194-195. doi: 10.1038/nrneurol.2018.18. Epub 2018 Feb 16. Nat Rev Neurol. 2018. PMID: 29449698 No abstract available.
-
Mehr Herz- und Hirninfarkte bei Migränikern.MMW Fortschr Med. 2018 Jun;160(11):32. doi: 10.1007/s15006-018-0620-z. MMW Fortschr Med. 2018. PMID: 29892862 German. No abstract available.
References
-
- Lipton RB, Bigal ME. The epidemiology of migraine. Am J Med 2005;118(Suppl 1):3S-10S. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous