

Cancer risk associated with chronic diseases and disease markers: prospective cohort study
- PMID: 29386192
- PMCID: PMC5791146
- DOI: 10.1136/bmj.k134
Cancer risk associated with chronic diseases and disease markers: prospective cohort study
Abstract
Objectives: To assess the independent and joint associations of major chronic diseases and disease markers with cancer risk and to explore the benefit of physical activity in reducing the cancer risk associated with chronic diseases and disease markers.
Design: Prospective cohort study.
Setting: Standard medical screening program in Taiwan.
Participants: 405 878 participants, for whom cardiovascular disease markers (blood pressure, total cholesterol, and heart rate), diabetes, chronic kidney disease markers (proteinuria and glomerular filtration rate), pulmonary disease, and gouty arthritis marker (uric acid) were measured or diagnosed according to standard methods, were followed for an average of 8.7 years.
Main outcome measures: Cancer incidence and cancer mortality.
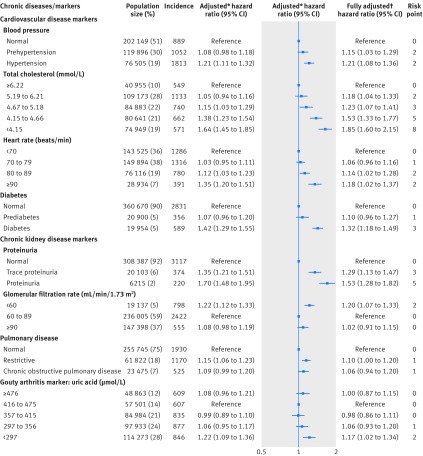
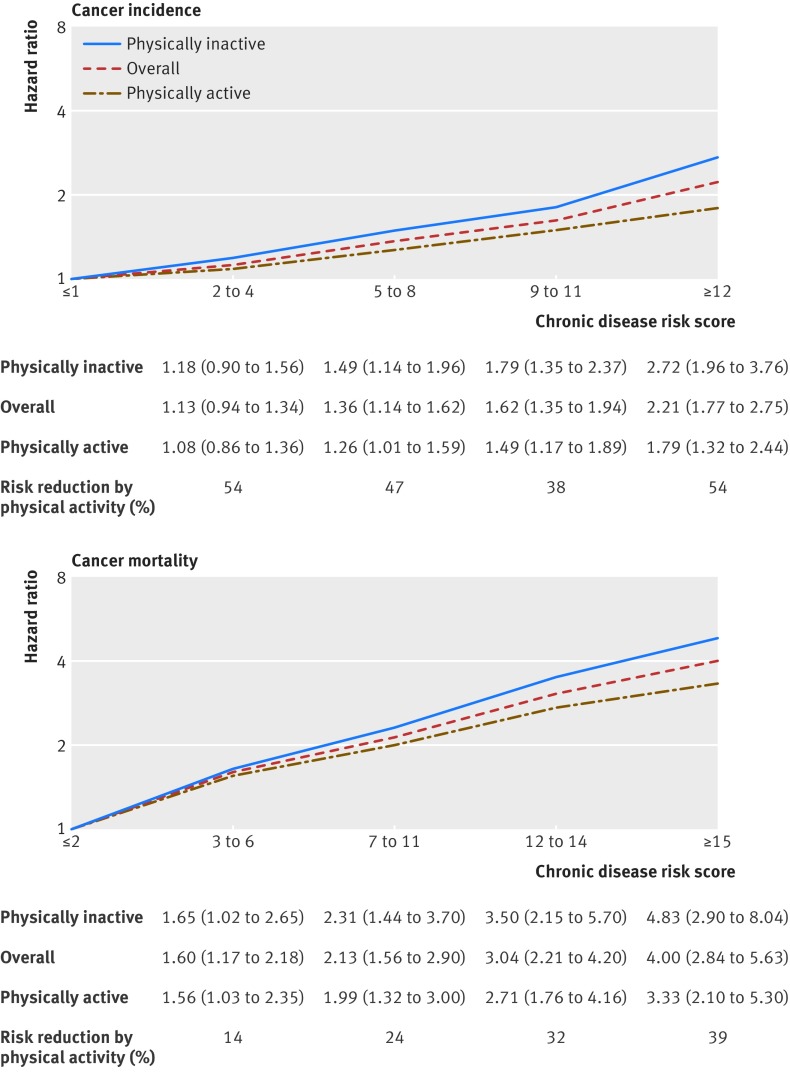
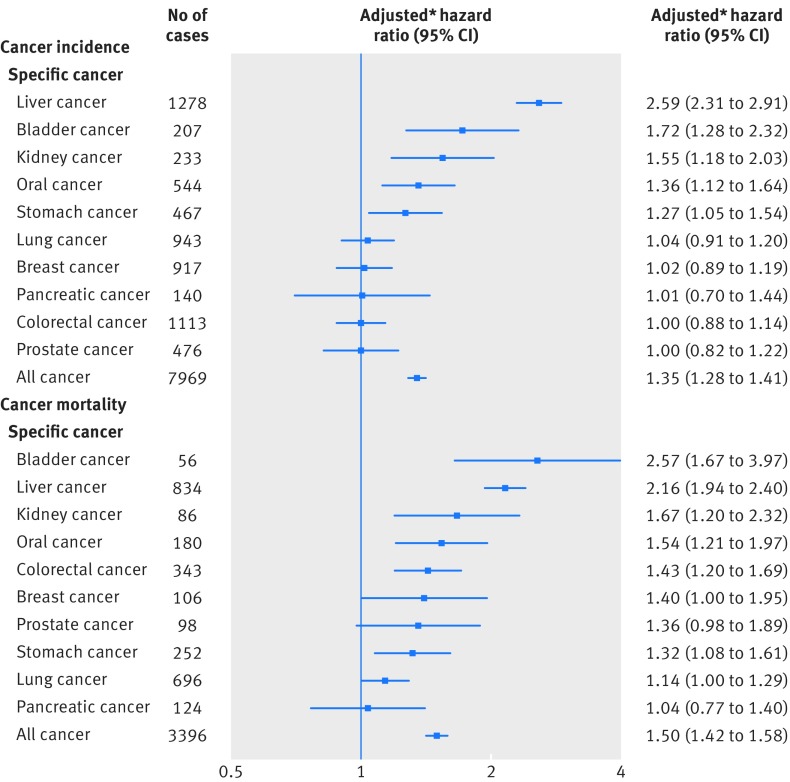
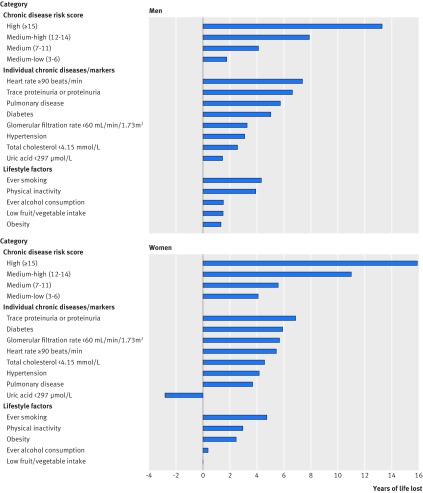
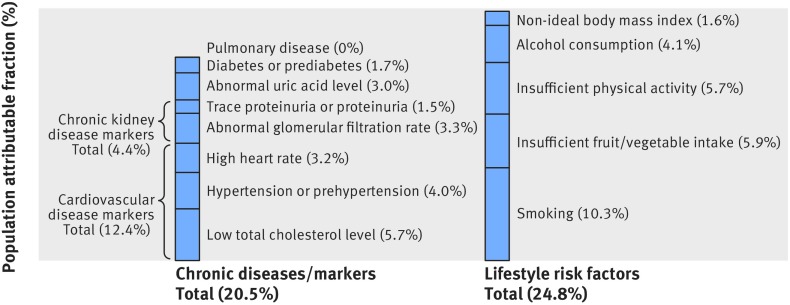
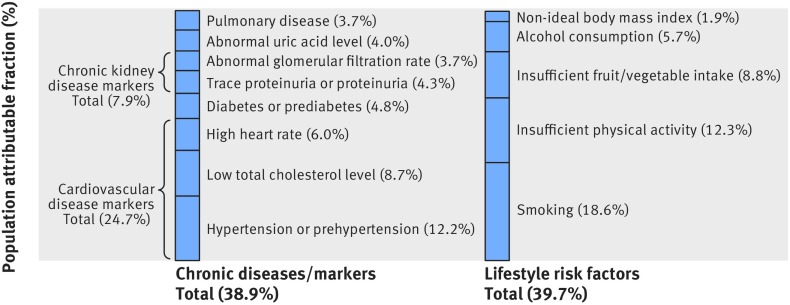
Results: A statistically significantly increased risk of incident cancer was observed for the eight diseases and markers individually (except blood pressure and pulmonary disease), with adjusted hazard ratios ranging from 1.07 to 1.44. All eight diseases and markers were statistically significantly associated with risk of cancer death, with adjusted hazard ratios ranging from 1.12 to 1.70. Chronic disease risk scores summarizing the eight diseases and markers were positively associated with cancer risk in a dose-response manner, with the highest scores associated with a 2.21-fold (95% confidence interval 1.77-fold to 2.75-fold) and 4.00-fold (2.84-fold to 5.63-fold) higher cancer incidence and cancer mortality, respectively. High chronic disease risk scores were associated with substantial years of life lost, and the highest scores were associated with 13.3 years of life lost in men and 15.9 years of life lost in women. The population attributable fractions of cancer incidence or cancer mortality from the eight chronic diseases and markers together were comparable to those from five major lifestyle factors combined (cancer incidence: 20.5% v 24.8%; cancer mortality: 38.9% v 39.7%). Among physically active (versus inactive) participants, the increased cancer risk associated with chronic diseases and markers was attenuated by 48% for cancer incidence and 27% for cancer mortality.
Conclusions: Chronic disease is an overlooked risk factor for cancer, as important as five major lifestyle factors combined. In this study, chronic diseases contributed to more than one fifth of the risk for incident cancer and more than one third of the risk for cancer death. Physical activity is associated with a nearly 40% reduction in the cancer risk associated with chronic diseases.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures


References
-
- GBD 2015 Mortality and Causes of Death Collaborators Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388:1459-544. 10.1016/S0140-6736(16)31012-1. - DOI - PMC - PubMed
-
- GBD 2013 Mortality and Causes of Death Collaborators Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015;385:117-71. 10.1016/S0140-6736(14)61682-2. - DOI - PMC - PubMed
-
- Stewart BW, Kleihues P (Eds). World Cancer Report 2014. IARCPress. Lyon 2014.
-
- Cancer Control: Knowledge into Action: WHO Guide for Effective Programmes: Module 2: Prevention. Geneva: World Health Organization 2007. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical