

Direct Repair of Localized Aortic Dissection with Critical Malperfusion of the Left Main Trunk
- PMID: 29386473
- PMCID: PMC6300423
- DOI: 10.5761/atcs.cr.17-00140
Direct Repair of Localized Aortic Dissection with Critical Malperfusion of the Left Main Trunk
Abstract
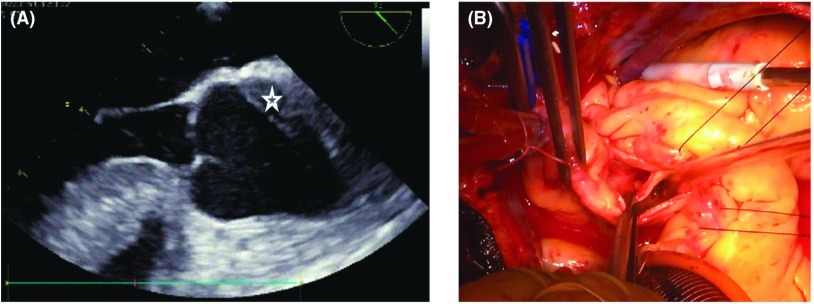
Background: Localized aortic dissection on the left coronary cusp with critical malperfusion of the left main trunk (LMT) is rare and carries a high risk of death.
Case presentation: We report a case of a 48-year-old patient who developed localized aortic dissection of the left coronary cusp complicated by critical malperfusion of the LMT of the coronary artery. After percutaneous coronary intervention (PCI) for the LMT, a Koster-Collins-like direct repair of the localized aortic dissection was carried out by closure of the false channel using BioGlue (CyroLife, Inc., Kennesaw, GA, USA) with the reinforcement of double Teflon felt strips.
Conclusion: The aortic repair using a modified Koster-Collins technique was successful.
Keywords: direct repair; localized aortic dissection; malperfusion of left main trunk.
Figures


References
-
- Masuyama S, Komiya T, Tamura N, et al. [Coronary malperfusion of left main trunk due to localized dissection of the ascending aorta]. Kyobu Geka 2007; 60: 433-7; discussion 437-40 (in Japanese) - PubMed
-
- Neri E, Toscano T, Papalia U, et al. Proximal aortic dissection with coronary malperfusion: presentation, management, and outcome. J Thorac Cardiovasc Surg 2001; 121: 552-60. - PubMed
-
- Murray CA, Edwards JE. Spontaneous laceration of ascending aorta. Circulation 1973; 47: 848-58. - PubMed
-
- Motallebzadeh R, Batas D, Valencia O, et al. The role of coronary angiography in acute type A aortic dissection. Eur J Cardiothorac Surg 2004; 25: 231-5. - PubMed
-
- Imoto K, Uchida K, Suzuki S, et al. Stenting of a left main coronary artery dissection and stent-graft implantation for acute type A aortic dissection. J Endovasc Ther 2005; 12: 258-61. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous