

Evaluation of Weight Loss Indicators and Laparoscopic One-Anastomosis Gastric Bypass Outcomes
- PMID: 29386655
- PMCID: PMC5792492
- DOI: 10.1038/s41598-018-20303-6
Evaluation of Weight Loss Indicators and Laparoscopic One-Anastomosis Gastric Bypass Outcomes
Erratum in
-
Author Correction: Evaluation of Weight Loss Indicators and Laparoscopic One-Anastomosis Gastric Bypass Outcomes.Sci Rep. 2018 Apr 26;8(1):6821. doi: 10.1038/s41598-018-24175-8. Sci Rep. 2018. PMID: 29700381 Free PMC article.
Abstract
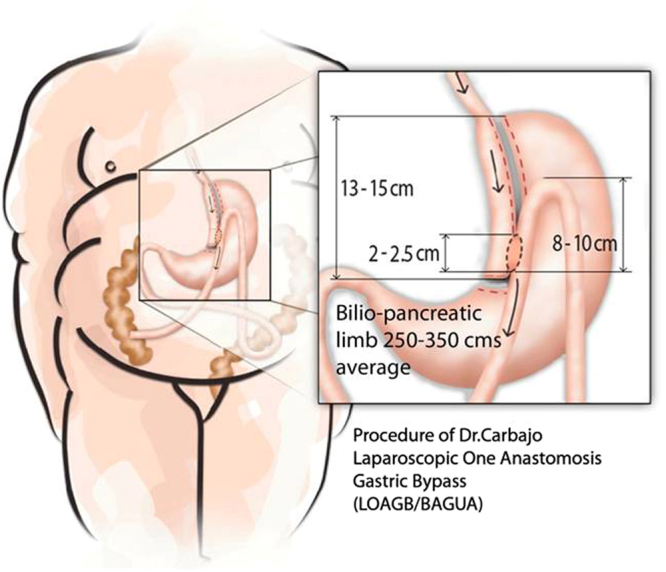
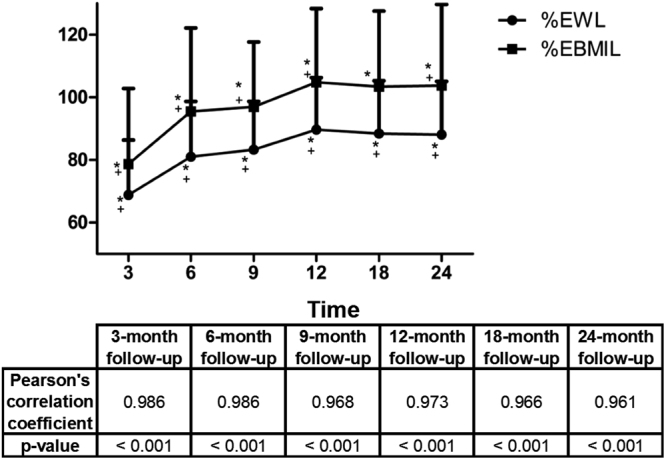
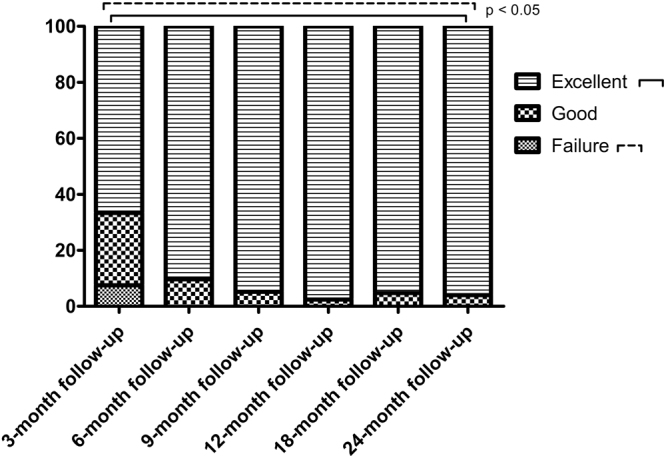
Mini-gastric bypass/One-anastomosis gastric bypass (MGB-OAGB) is an effective bariatric technique for treating overweight and obesity, controlling and improving excess-weight-related comorbidities. Our study evaluated OAGB characteristics and resulting weight evolution, plus surgical success criteria based on various excess weight loss indicators. A prospective observational study of 100 patients undergoing OAGB performed by the same surgical team (two-year follow-up). Surgical characteristics were: surgery duration, associated complications, bowel loop length, hospital stay, and weight loss at 6 postoperative points. 100 patients were treated (71 women, 29 men); mean initial age was 42.61 years and mean BMI, 42.61 ± 6.66 kg/m2. Mean surgery duration was 97.84 ± 12.54 minutes; biliopancreatic loop length was 274.95 ± 23.69 cm. Average hospital stay was 24 hours in 98% of patients; no surgical complications arose. Weight decreased significantly during follow-up (P < 0.001). Greatest weight loss was observed at 12 months postsurgery (68.56 ± 13.10 kg). Relative weight loss showed significant positive correlation, with greatest weight loss at 12 months and %excess BMI loss > 50% achieved from the 3-month follow-up in 92.46% of patients. OAGB seems to be effective in treating obesity, with short hospital stays. Relative weight loss correlates optimally with absolute outcomes, but both measures should be used to evaluate surgical results.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization; WHO. Global Health Observatory data. Web site http://www.who.int/mediacentre/factsheets/fs311/es/ (2016).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
