

Intraoral radiographic tips and tricks
Affiliations
- PMID: 29386685
- PMCID: PMC5764209
Item in Clipboard
Intraoral radiographic tips and tricks
Can Vet J.
2018 Feb.
No abstract available
Figures

Disposable contamination barrier sleeve over X-ray tube head.

Disposable contamination barrier sheet over control panel on X-ray generator.

Top, a box of air/water syringe covers. Bottom right, a box of latex finger cots. Bottom left, the digital dental X-ray sensor in its natural state.

The digital dental X-ray sensor all dressed and ready for action.

A radiograph of the left caudal maxilla of a dog with a great deal of contamination on the sensor plate, resulting in a non-diagnostic image (waste of time, money, and radiation exposure).

A bisecting angle view of the right maxilla in a dog skull after removal of the 4th premolar tooth and placement of a radiodense object in either the mesiobuccal or palatal sockets. How can we determine where this errant “root” is located?

That same area as viewed using the occlusal view. Now it is very apparent that the “root” is hiding in the palatal socket. Identifying where the root tip is is the first step in removing it.

Occlusal view of the right maxilla of a Pekinese dog following extraction of the remaining teeth. But wait, there are remains of the mesial and distal roots of the 1st molar tooth still clearly present in their sockets.

Occlusal view of the same dog after retrieval of the retained root remnants. Now that their complete removal has been confirmed and documented, the wound can be closed.
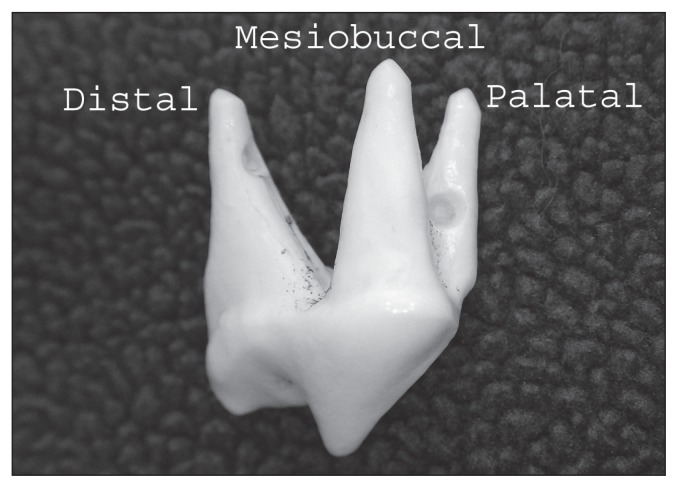
Plastic model of the right upper 4th premolar tooth in a dog identifying the three roots.

My right hand acting as an analog for a right maxillary 4th premolar tooth. My thumb represents the distal root, my index finger represents the mesiobuccal root, and my second finger (which cannot be seen because it is hidden behind my index finger), represents the palatal root.

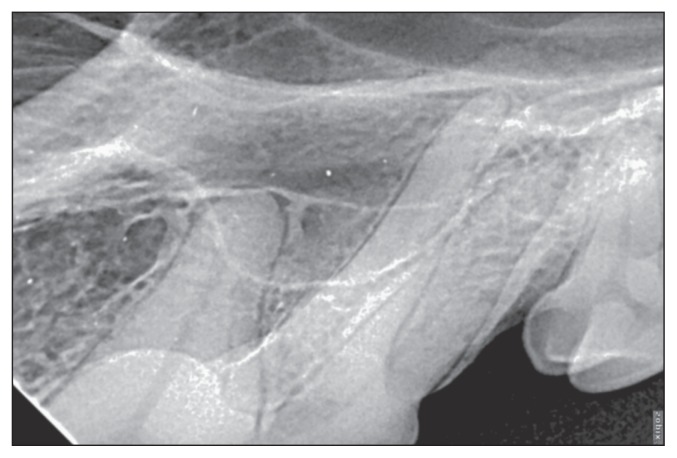
A radiograph of a right maxillary 4th premolar tooth with a clear view of the distal root to the left and mesiobuccal and palatal roots superimposed one over the other to the right. In this view, neither of those roots can be seen clearly.

I have moved my head (camera) to the left, mimicking a caudal to rostral oblique projection. As my head moved left, it appears that my second finger (the palatal root) also moved to the left and we can now see it between the other two “roots.”
A radiograph of the right maxillary fourth premolar tooth in a dog shot in a caudal to rostral oblique direction. From left to right we see the distal root, the palatal root and the mesiobuccal root.

Here I have moved my head (camera) to the right, mimicking a rostral to caudal oblique projection and my second finger (palatal root) is now visible to the right of my index finger (mesiobuccal root).

A radiograph of the right maxillary fourth premolar tooth shot in a rostral to caudal projection. From left to right we see the distal root (partially hidden behind the first molar tooth), the mesiobuccal root and the palatal root.

A dry bone cat skull with a PSP sensor plate (left out of its contamination barrier sleeve for visual clarity) placed against the palatal side of the down-side (left teeth) and parallel to the crowns of the up-side (right teeth). The X-ray tube head is angled “almost parallel” to both with the objective being for the beams to sneak under the arch to give a relatively clear view of the teeth.

A view of the right maxilla in a cat using the “almost parallel” technique. The zygomatic are is visible but so are all roots of these teeth.

This parallel technique view of the left mandible in a mature pug does not really make it clear if the third molar is present or not.

This caudal to rostral oblique view in the same dog demonstrated that the third molar was present, mal-oriented and unerupted. Such a tooth is at risk for the development of a dentigerous cyst and should be removed.

An image of the left mandibular premolars with the label positioned away from any diagnostically useful information. The use of the patient ID number lets me know who this is but I can still share it without violating client confidentiality.

A partial study (on analog film) of a 5-year-old toy poodle with massive periodontal disease. The images have been oriented and arranged in the proper fashion with the dog’s right teeth to our left, left teeth to our right, upper teeth pointing down and lower teeth pointing up.
MeSH terms
LinkOut - more resources
Full Text Sources