

Predictors of pneumonia on routine chest radiographs in patients with COPD: a post hoc analysis of two 1-year randomized controlled trials
- PMID: 29386888
- PMCID: PMC5764287
- DOI: 10.2147/COPD.S142530
Predictors of pneumonia on routine chest radiographs in patients with COPD: a post hoc analysis of two 1-year randomized controlled trials
Abstract
Background: Patients with COPD are at risk for life-threatening pneumonia. Although anatomical abnormalities in the thorax may predispose to pneumonia, those abnormalities identified on routine chest X-rays (CXRs) in patients with COPD have not been studied to better understand pneumonia risk.
Methods: We conducted a post hoc exploratory analysis of data from two replicate year-long clinical trials assessing the impact of fluticasone furoate-vilanterol versus vilanterol alone on COPD exacerbations (GSK studies: HZC102871/NCT01009463 and HZC102970/NCT01017952). Abnormalities on baseline CXRs from 179 patients who developed pneumonia and 50 randomly selected patients who did not were identified by blinded consensus readings conducted by two radiologists. Positive and negative likelihood ratios and diagnostic odds ratios (ORs) were calculated to evaluate the markers for subsequent pneumonia development during the 1-year study period.
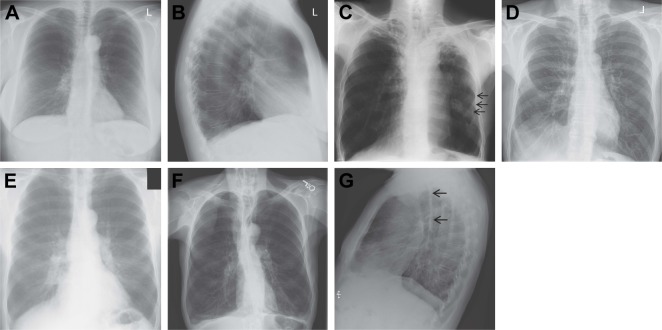
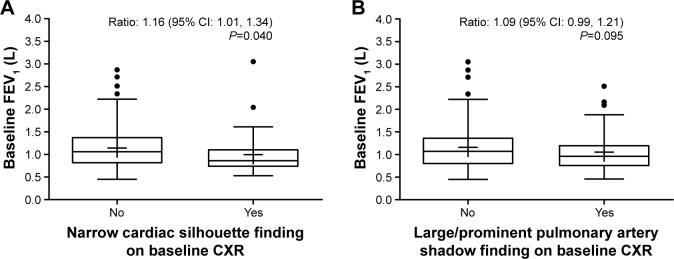
Results: Baseline characteristics distinguishing the pneumonia and non-pneumonia groups included a lower body mass index (24.9 vs 27.5 kg/m2, P=0.008), more severe airflow obstruction (mean post-bronchodilator forced expiratory volume in 1 second [FEV1]/forced vital capacity ratio: 42.3% vs 47.6%, P=0.003), and prior pneumonia (36% vs 20%, P=0.030). Baseline CXR findings with the highest diagnostic ORs were: elevated hemi-diaphragm (OR: 6.87; 95% CI: 0.90, 52.26), thick tracheal-esophageal stripe (OR: 4.39 [0.25, 78.22]), narrow cardiac silhouette (OR: 2.91 [0.85, 9.99]), calcified pleural plaque/mid-chest pleural thickening (OR: 2.82 [0.15, 53.76]), and large/prominent pulmonary artery shadow (OR: 1.94 [0.95, 3.97]). The presence of a narrow cardiac silhouette at baseline was associated with a statistically significant lower mean pre-bronchodilator FEV1 (P=0.040). There was also a trend for a lower mean pre-bronchodilator FEV1 in patients with a large/prominent pulmonary artery shadow at baseline (P=0.095).
Conclusion: Findings on routine CXR that relate to pathophysiological mechanisms of pneumonia could help determine pneumonia risk in patients with COPD.
Keywords: COPD; chest X-rays; pneumonia; predictors of risk.
Conflict of interest statement
Disclosure DBR, SL, DVG, and CC: employment and stock ownership (GSK). SB: employment (GSK) at the time the analysis was conducted. HAA: employment and shareholder (Bristol-Myers Squibb). The current affiliation for HAA is Headquarters Medical, Immunoscience Marketed Products Development, Bristol-Myers Squibb, Princeton, NJ, USA. The authors report no other conflicts of interest in this work.
Figures
References
-
- Curcio D, Cané A, Isturiz R. Redefining risk categories for pneumococcal disease in adults: critical analysis of the evidence. Int J Infect Dis. 2015;37:30–35. - PubMed
-
- Crim C, Calverley PM, Anderson JA, et al. Pneumonia risk in COPD patients receiving inhaled corticosteroids alone or in combination: TORCH study results. Eur Respir J. 2009;34(3):641–647. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
