

Relationship between exercise endurance and static hyperinflation in a post hoc analysis of two clinical trials in patients with COPD
- PMID: 29386889
- PMCID: PMC5764300
- DOI: 10.2147/COPD.S145285
Relationship between exercise endurance and static hyperinflation in a post hoc analysis of two clinical trials in patients with COPD
Abstract
Background: Lung hyperinflation and exercise intolerance are hallmarks of chronic obstructive pulmonary disease (COPD). However, their relationship remains uncertain. A combined analysis of two placebo-controlled, randomized studies examined the effects of the long-acting muscarinic antagonist umeclidinium (UMEC) and long-acting β2-agonist vilanterol (VI) separately and in combination on static hyperinflation, exercise endurance time (EET), and their relationship in patients with COPD.
Methods: Patients with moderate-to-severe stable COPD and resting functional residual capacity >120% predicted were randomized to UMEC/VI 62.5/25 μg, UMEC 62.5 μg, VI 25 μg, or placebo for 12 weeks. Inspiratory capacity (IC), residual volume (RV), total lung capacity (TLC), and EET in an endurance shuttle-walk test were measured. In this post hoc analysis, IC/TLC, RV/TLC, and IC were used as hyperinflation markers.
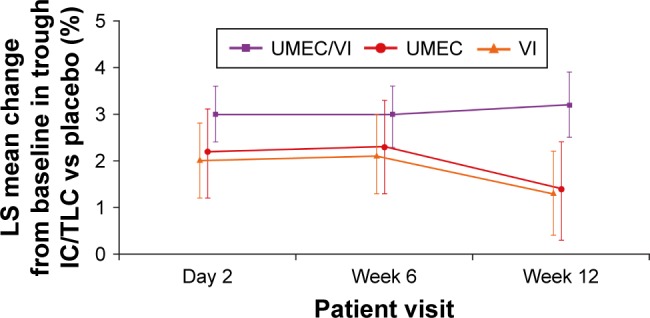
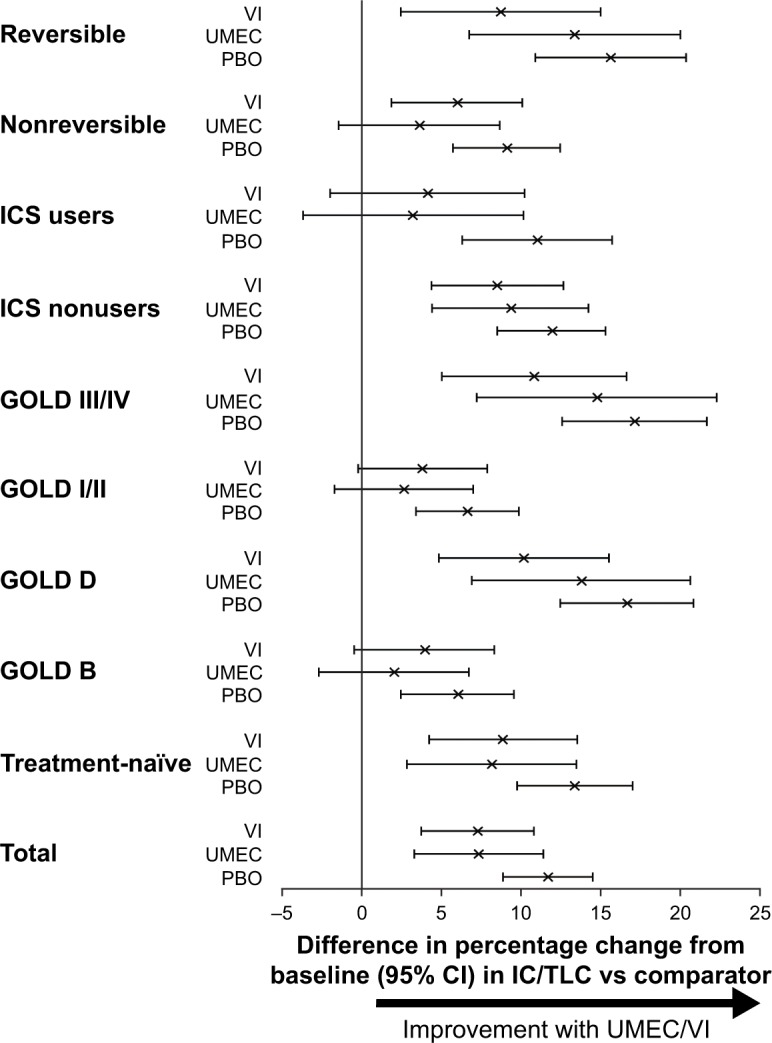
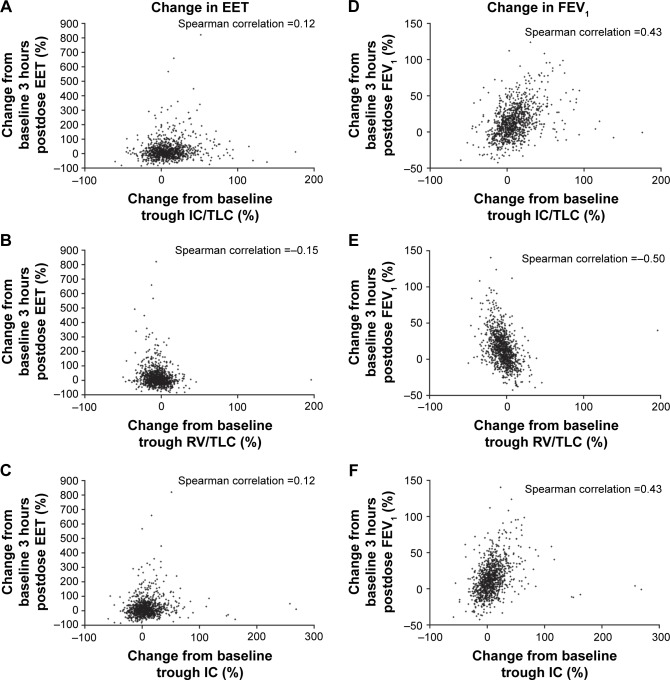
Results: After 12 weeks, UMEC/VI and UMEC and VI showed significant improvements in hyperinflation versus placebo when measured by absolute change from baseline in IC/TLC (trough and 3 hours postdose [P≤0.011]). UMEC/VI showed significant improvements versus UMEC and VI in absolute changes in IC/TLC (trough and 3 hours postdose [P≤0.001]). Statistical significance for comparisons with placebo and between treatments for absolute changes in IC and percentage changes in RV/TLC followed similar patterns to those for absolute changes in IC/TLC. UMEC/VI showed significant improvements in EET versus placebo at day 2 and week 12, measured as change from baseline in seconds (P≤0.002) and as a percentage from baseline (P≤0.005). There was a lack of evidence to suggest a correlation between improvements in static hyperinflation and EET at any time point.
Conclusion: Although the dual bronchodilator UMEC/VI demonstrated greater improvements in static hyperinflation markers than UMEC or VI and significant improvements in exercise endurance, no direct relationship was observed between static hyperinflation and exercise endurance.
Keywords: COPD; bronchodilators; exercise; hyperinflation.
Conflict of interest statement
Disclosure SS was supported by the Collaboration for Leadership in Applied Health Research and Care (CLAHRC) East Midlands and the National Institute for Health Research (NIHR) Leicester Biomedical Research Centre. The views expressed are those of the author(s), and not necessarily those of the National Health Service (NHS), NIHR, or Department of Health. SS was also involved in the development of the endurance shuttle-walk test, and has served on advisory boards for AstraZeneca, GSK, and Novartis. FM has received fees for speaking at conferences sponsored by Boehringer Ingelheim, Grifols, and Novartis, research grants for participating in multicenter trials sponsored by AstraZeneca, Boehringer Ingelheim, GSK, and Novartis, and unrestricted research grants from Boehringer Ingelheim and Novartis. FM holds a Canadian Institutes of Health Research (CIHR)/GSK research chair on COPD. LT is a contingent worker on assignment at GSK. WAF, MVB, NL, and JHR are employees of GSK and hold stock/shares in GSK. The authors report no other conflicts of interest in this work.
Figures
References
-
- Zanen P, Rutten F, Hoes A, Lammers J. Prevalence of hyperinflation in COPD and correlation with flow-volume indices. Chest. 2005;128(4 Suppl):132S–133S.
-
- O’Donnell DE, Laveneziana P. Physiology and consequences of lung hyperinflation in COPD. Eur Respir Rev. 2006;15(100):61–67.
-
- Oh YM, Sheen SS, Park JH, et al. Emphysematous phenotype is an independent predictor for frequent exacerbation of COPD. Int J Tuberc Lung Dis. 2014;18(12):1407–1414. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
