

Phenotyping COPD exacerbations using imaging and blood-based biomarkers
- PMID: 29386890
- PMCID: PMC5764289
- DOI: 10.2147/COPD.S152484
Phenotyping COPD exacerbations using imaging and blood-based biomarkers
Abstract
Rationale: Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are caused by a variety of different etiologic agents. Our aim was to phenotype COPD exacerbations using imaging (chest X-ray [CXR] and computed tomography [CT]) and to determine the possible role of the blood tests (C-reactive protein [CRP], the N-terminal prohormone brain natriuretic peptide [NT-proBNP]) as diagnostic biomarkers.
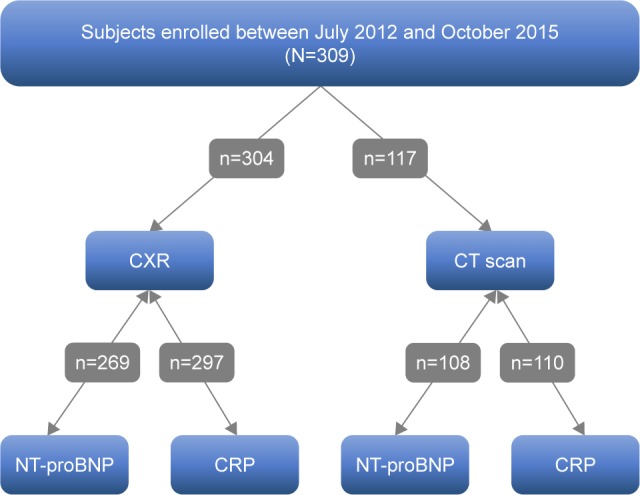
Materials and methods: Subjects who were hospitalized with a primary diagnosis of AECOPD and who had had CXRs, CT scans, and blood collection for CRP and NT-proBNP were assessed in this study. Radiologist blinded to the clinical and laboratory characteristics of the subjects interpreted their CXRs and CT images. ANOVA and Spearman's correlation were performed to test for associations between these imaging parameters and the blood-based biomarkers NT-proBNP and CRP; logistic regression models were used to assess the performance of these biomarkers in predicting the radiological parameters.
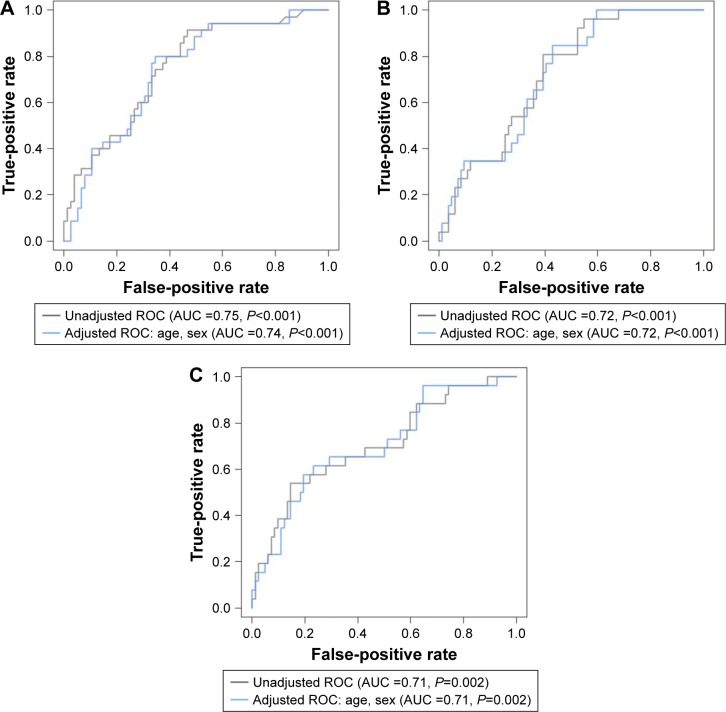
Results: A total of 309 subjects were examined for this study. Subjects had a mean age of 65.6±11.1 years, 66.7% of them were males, and 62.4% were current smokers, with a mean FEV1 54.4%±21.5% of predicted. Blood NT-proBNP concentrations were associated with cardiac enlargement (area under the curve [AUC] =0.72, P<0.001), pulmonary edema (AUC =0.63, P=0.009), and pleural effusion on CXR (AUC =0.64, P=0.01); whereas on CT images, NT-proBNP concentrations were associated with pleural effusion (AUC =0.71, P=0.002). Serum CRP concentrations, on the other hand, were associated with consolidation on CT images (AUC =0.75, P<0.001), ground glass opacities (AUC =0.64, P=0.028), and pleural effusion (AUC =0.72, P<0.001) on CT images. A serum CRP sensitivity-oriented cutoff point of 11.5 mg/L was selected for the presence of consolidation on CT images in subjects admitted as cases of AECOPD, which has a sensitivity of 91% and a specificity of 53% (P<0.001).
Conclusion: Elevated CRP may indicate the presence of pneumonia, while elevated NT-proBNP may indicate cardiac dysfunction. These readily available blood-based biomarkers may provide more accurate phenotyping of AECOPD and enable the discovery of more precise therapies.
Keywords: CT scan; biomarker; chest X-ray; chronic obstructive pulmonary disease; exacerbation.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
Similar articles
-
C-reactive protein and N-terminal prohormone brain natriuretic peptide as biomarkers in acute exacerbations of COPD leading to hospitalizations.PLoS One. 2017 Mar 22;12(3):e0174063. doi: 10.1371/journal.pone.0174063. eCollection 2017. PLoS One. 2017. PMID: 28328968 Free PMC article.
-
N-Terminal Prohormone of Brain Natriuretic Peptide (NT-proBNP) as a Diagnostic Biomarker of Left Ventricular Systolic Dysfunction in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD).Lung. 2018 Oct;196(5):583-590. doi: 10.1007/s00408-018-0137-3. Epub 2018 Jun 27. Lung. 2018. PMID: 29951921
-
Association of left-heart dysfunction with severe exacerbation of chronic obstructive pulmonary disease: diagnostic performance of cardiac biomarkers.Am J Respir Crit Care Med. 2006 Nov 1;174(9):990-6. doi: 10.1164/rccm.200603-380OC. Epub 2006 Jul 13. Am J Respir Crit Care Med. 2006. PMID: 16840745
-
The clinical value of suPAR in diagnosis and prediction for patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis.Ther Adv Respir Dis. 2020 Jan-Dec;14:1753466620938546. doi: 10.1177/1753466620938546. Ther Adv Respir Dis. 2020. PMID: 32643535 Free PMC article.
-
Recent Advances in Computed Tomography Imaging in Chronic Obstructive Pulmonary Disease.Ann Am Thorac Soc. 2018 Mar;15(3):281-289. doi: 10.1513/AnnalsATS.201705-377FR. Ann Am Thorac Soc. 2018. PMID: 28812906 Free PMC article. Review.
Cited by
-
Awareness and barriers of adherence to chronic obstructive pulmonary disease guidelines among respiratory therapists.Ann Thorac Med. 2025 Apr-Jun;20(2):108-116. doi: 10.4103/atm.atm_227_24. Epub 2025 Mar 31. Ann Thorac Med. 2025. PMID: 40236381 Free PMC article.
-
Phenotyping and outcomes of hospitalized COPD patients using rapid molecular diagnostics on sputum samples.Int J Chron Obstruct Pulmon Dis. 2019 Jan 23;14:311-319. doi: 10.2147/COPD.S188186. eCollection 2019. Int J Chron Obstruct Pulmon Dis. 2019. PMID: 30774328 Free PMC article.
-
Treatable traits in acute exacerbations of chronic airway diseases.Chron Respir Dis. 2019 Jan-Dec;16:1479973119867954. doi: 10.1177/1479973119867954. Chron Respir Dis. 2019. PMID: 31409129 Free PMC article. Review.
-
Differential Diagnosis of Suspected Chronic Obstructive Pulmonary Disease Exacerbations in the Acute Care Setting: Best Practice.Am J Respir Crit Care Med. 2023 May 1;207(9):1134-1144. doi: 10.1164/rccm.202209-1795CI. Am J Respir Crit Care Med. 2023. PMID: 36701677 Free PMC article. Review.
-
Increased Serum Soluble Interleukin-2 Receptor Associated with Severity of Acute Exacerbation of Chronic Obstructive Pulmonary Disease.Int J Chron Obstruct Pulmon Dis. 2021 Sep 7;16:2561-2573. doi: 10.2147/COPD.S321904. eCollection 2021. Int J Chron Obstruct Pulmon Dis. 2021. PMID: 34522094 Free PMC article.
References
-
- Perera PN, Armstrong EP, Sherrill DL, Skrepnek GH. Acute exacerbations of COPD in the United States: inpatient burden and predictors of costs and mortality. COPD. 2012;9(2):131–141. - PubMed
-
- Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am J Respir Crit Care Med. 2017;195(5):557–582. - PubMed
-
- Zdravkovic V, Mladenovic V, Colic M, et al. NT-proBNP for prognostic and diagnostic evaluation in patients with acute coronary syndromes. Kardiol Pol. 2013;71(5):472–479. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
