

Safety aspects of hysteroscopy, specifically in relation to entry and specimen retrieval: a UK survey of practice
- PMID: 29386987
- PMCID: PMC5769820
- DOI: 10.1186/s10397-018-1036-6
Safety aspects of hysteroscopy, specifically in relation to entry and specimen retrieval: a UK survey of practice
Abstract
Background: The purpose of this study is to evaluate current practice amongst gynaecologists across the UK, regarding safety aspects of inpatient hysteroscopy under anaesthesia, specifically in relation to entry and specimen retrieval.A survey was created using survey monkey. The first round was circulated to all registrar trainees and consultant gynaecologists across Wales. Following a good response, the survey was then circulated to all members of the British Society of Gynaecological Endoscopy (BSGE).
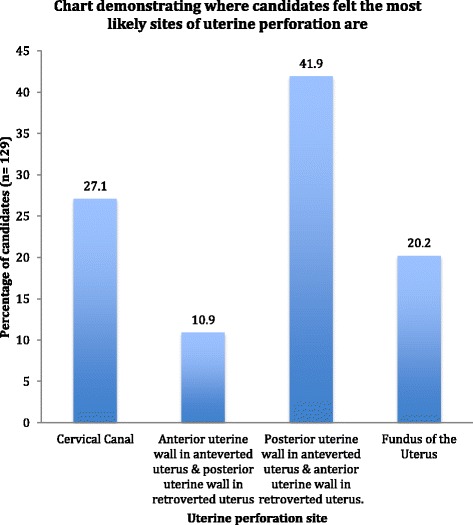
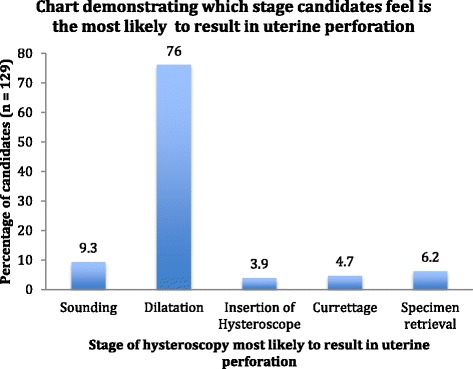
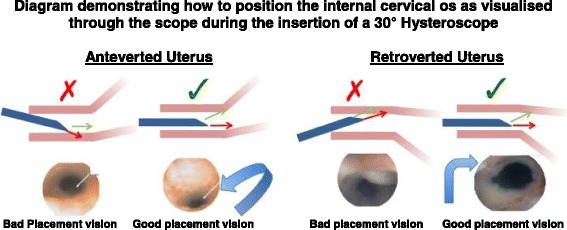
Results: There were 212 responses including, 140 consultants, 36 senior registrars, 17 junior registrars and 18 clinical nurse specialists. In total, 136 out of 212 (64.7%) always perform a vaginal examination prior to hysteroscopy. 10.4% always sound the uterus, and 5.2% always dilate the uterus prior to insertion of the hysteroscope. Twenty-three consultants, six senior registrars, three junior registrars and one clinical nurse specialist knew how to position the internal cervical os as visualised through the scope when using a 30° hysteroscope. 35.8% of candidates always perform a post-procedure cavity check, and 9% use suction to flush the cavity to aid vision during the post-procedure cavity check. The majority (76%) predicted dilatation as the stage most likely to cause uterine perforation and predicted the most likely site for perforation as the posterior uterine wall in the anteverted uterus and the anterior uterine wall in the retroverted uterus.
Conclusion: This study highlights varied practice across the UK regarding safety aspects of hysteroscopy, in relation to entry and specimen retrieval. There is a need for increased awareness of the risks of hysteroscopy and paramount precautions that should be performed routinely as part of their practice. Standardised guidelines may be a beneficial tool to help bring about this change in practice, leading to a reduction in uterine perforation rates.
Keywords: Hysteroscopy; Specimen retrieval; Uterine perforation.
Conflict of interest statement
No ethical approval was required as the survey was optional and anonymous and study aims explained to all candidates prior to performing the survey.Not applicable.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Building a sustainable rural physician workforce.Med J Aust. 2021 Jul;215 Suppl 1:S5-S33. doi: 10.5694/mja2.51122. Med J Aust. 2021. PMID: 34218436
-
Laparoscopic specimen retrieval and attitudes towards morcellation: a questionnaire survey of gynaecology consultants in the United Kingdom.J Obstet Gynaecol. 2019 Apr;39(3):345-348. doi: 10.1080/01443615.2018.1493096. Epub 2018 Nov 13. J Obstet Gynaecol. 2019. PMID: 30422734
-
Use of contact hysteroscopy in evaluating postpartum bleeding and incomplete abortion.J Reprod Med. 1984 Oct;29(10):749-51. J Reprod Med. 1984. PMID: 6334735
-
Complete and partial uterine perforation and embedding following insertion of intrauterine devices. II. Diagnostic methods, prevention, and management.Obstet Gynecol Surv. 1981 Aug;36(8):401-17. doi: 10.1097/00006254-198108000-00001. Obstet Gynecol Surv. 1981. PMID: 6455610 Review.
-
[Prevention of the complications related to hysteroscopy: guidelines for clinical practice].J Gynecol Obstet Biol Reprod (Paris). 2013 Dec;42(8):1032-49. doi: 10.1016/j.jgyn.2013.09.008. Epub 2013 Nov 7. J Gynecol Obstet Biol Reprod (Paris). 2013. PMID: 24210234 Review. French.
Cited by
-
Training in Diagnostic Hysteroscopy: The "Arbor Vitae" Method.Medicina (Kaunas). 2023 May 24;59(6):1019. doi: 10.3390/medicina59061019. Medicina (Kaunas). 2023. PMID: 37374222 Free PMC article.
References
-
- Jansen FW, et al. Complications of hysteroscopy: a prospective, multicenter study. Obstet Gynaecol J. 2000;96(2):266–270. - PubMed
-
- Best Practice in Outpatient Hysteroscopy . Green-top Guideline No. 59. 2011.
-
- Passini A, Belloni C. Intraoperative complications of 697 consecutive operative hysteroscopies. Minerva Gynaecol J. 2001;53(1):13–20. - PubMed
-
- Petrozza JC. Hysteroscopy Treatment & Management. In: Rivlin ME, editor. eMedicine.com. 2015.
LinkOut - more resources
Full Text Sources
Other Literature Sources