

Clinical characteristic and intraoperative findings of uterine perforation patients in using of intrauterine devices (IUDs)
- PMID: 29386988
- PMCID: PMC5770510
- DOI: 10.1186/s10397-017-1032-2
Clinical characteristic and intraoperative findings of uterine perforation patients in using of intrauterine devices (IUDs)
Abstract
Background: Intrauterine devices (IUDs) are the most popular form of contraception used worldwide; however, IUD is not risk-free. IUD migrations, especially uterine perforations, were frequently occurred in patients. The aim of this study was to investigate the clinical characteristics and intraoperative findings in patients with migrated IUDs.
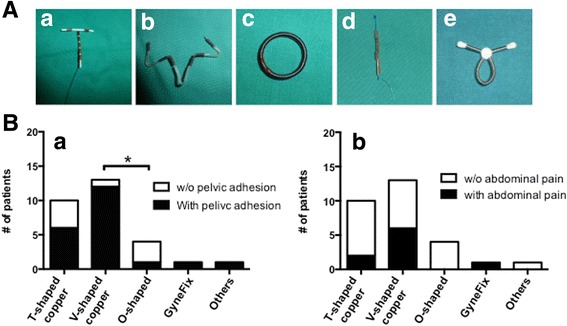
Results: 29 cases of uterine perforation associated with migrated IUDs and 69 control patients were followed between January 2008 to March 2015. Patients who used IUDs within first 6 months from the last delivery experienced a characteristically high rate of the perforation of the uterine wall. A significantly larger number of IUD insertion associated with uterine perforation were performed in rural hospitals or operated at a lower level health care system. There was no clear difference in the age and presented symptoms in patients between two groups. Majority of contraceptive intrauterine devices was the copper-releasing IUDs. Furthermore, patients who used V-shaped IUD showed significantly higher incidence of pelvic adhesions when compared with the users of O-shaped IUDs.
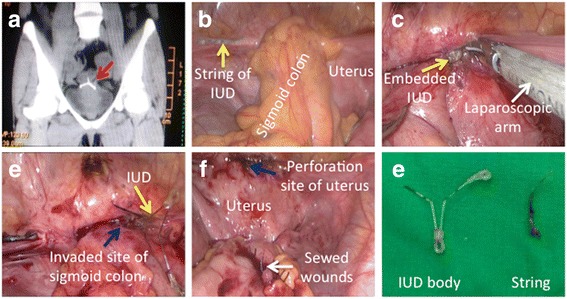
Conclusions: Unique clinical characteristics of IUD migration were identified in patients with uterine perforation. Hysteroscopy and/or laparoscopy were the effective approaches to remove the migrated IUDs. Improving operating skills is required at the lower level of health care system.
Keywords: Hysteroscopy; IUD; Laparoscopy; Uterine perforation.
Conflict of interest statement
This study was approved by the Review Board and Ethics Committee of the 3rd Xiangya Hospital of Central South University.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Uterine perforation by copper intrauterine device.Eur J Obstet Gynecol Reprod Biol. 1984 Jun;17(4):257-61. doi: 10.1016/0028-2243(84)90068-6. Eur J Obstet Gynecol Reprod Biol. 1984. PMID: 6378687
-
Intrauterine devices: an effective alternative to oral hormonal contraception.Prescrire Int. 2009 Jun;18(101):125-30. Prescrire Int. 2009. PMID: 19637436
-
Uterine perforation caused by intrauterine devices: clinical course and treatment.Hum Reprod. 2013 Jun;28(6):1546-51. doi: 10.1093/humrep/det074. Epub 2013 Mar 22. Hum Reprod. 2013. PMID: 23526304
-
Complete and partial uterine perforation and embedding following insertion of intrauterine devices. II. Diagnostic methods, prevention, and management.Obstet Gynecol Surv. 1981 Aug;36(8):401-17. doi: 10.1097/00006254-198108000-00001. Obstet Gynecol Surv. 1981. PMID: 6455610 Review.
-
Complete and partial uterine perforation and embedding following insertion of intrauterine devices. I. Classification, complications, mechanism, incidence, and missing string.Obstet Gynecol Surv. 1981 Jul;36(7):335-53. doi: 10.1097/00006254-198107000-00001. Obstet Gynecol Surv. 1981. PMID: 7029368 Review.
Cited by
-
Neglected Intrauterine Device Migration Complications: Case Reports.Womens Health Rep (New Rochelle). 2023 Jan 18;4(1):11-18. doi: 10.1089/whr.2022.0099. eCollection 2023. Womens Health Rep (New Rochelle). 2023. PMID: 36727094 Free PMC article.
-
Intrauterine device found in an ovarian tumor: A case report.Medicine (Baltimore). 2020 Oct 16;99(42):e22825. doi: 10.1097/MD.0000000000022825. Medicine (Baltimore). 2020. PMID: 33080762 Free PMC article.
-
Ectopic intrauterine device in the bladder causing cystolithiasis: A case report.World J Clin Cases. 2022 Apr 6;10(10):3194-3199. doi: 10.12998/wjcc.v10.i10.3194. World J Clin Cases. 2022. PMID: 35611133 Free PMC article.
-
Four cases of heterotopia of an intrauterine device embedded in the bladder muscular layer causing cystolithiasis: case report and review of the literature.J Int Med Res. 2021 Jan;49(1):300060520979444. doi: 10.1177/0300060520979444. J Int Med Res. 2021. PMID: 33472467 Free PMC article. Review.
-
Evaluation of pharmacokinetics and safety of a long-term estradiol-releasing stent in rat uterine.Regen Ther. 2022 Oct 21;21:494-501. doi: 10.1016/j.reth.2022.10.001. eCollection 2022 Dec. Regen Ther. 2022. PMID: 36313395 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources