

Provision of emergency obstetric care at secondary level in a conflict setting in a rural area of Afghanistan - is the hospital fulfilling its role?
- PMID: 29387145
- PMCID: PMC5776770
- DOI: 10.1186/s13031-018-0137-1
Provision of emergency obstetric care at secondary level in a conflict setting in a rural area of Afghanistan - is the hospital fulfilling its role?
Abstract
Background: Provision of Emergency Obstetric and Neonatal Care (EmONC) reduces maternal mortality and should include three components: Basic Emergency Obstetric and Neonatal Care (BEmONC) offered at primary care level, Comprehensive EmONC (CEmONC) at secondary level and a good referral system in-between. In a conflict-affected province of Afghanistan (Khost), we assessed the performance of an Médecins Sans Frontières (MSF) run CEmONC hospital without a primary care and referral system. Performance was assessed in terms of hospital utilisation for obstetric emergencies and quality of obstetric care.
Methods: A cross-sectional study using routine programme data (2013-2014).
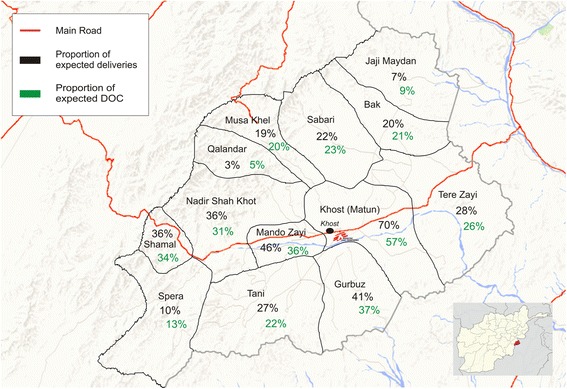
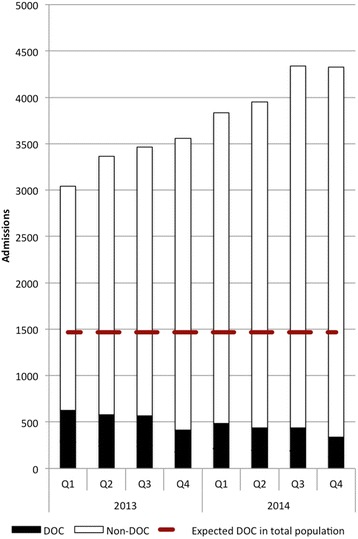
Results: Of 29,876 admissions, 99% were self-referred, 0.4% referred by traditional birth attendants and 0.3% by health facilities. Geographic origins involved clustering around the hospital vicinity and the provincial road axis. While there was a steady increase in hospital caseload, the number and proportion of women with Direct Obstetric Complications (DOC) progressively dropped from 21% to 8% over 2 years. Admissions for normal deliveries continuously increased. In-hospital maternal deaths were 0.03%, neonatal deaths 1% and DOC case-fatality rate 0.2% (all within acceptable limits).
Conclusions: Despite a high and ever increasing caseload, good quality Comprehensive EmONC could be offered in a conflict-affected setting in rural Afghanistan. However, the primary emergency role of the hospital is challenged by diversion of resources to normal deliveries that should happen at primary level. Strengthening Basic EmONC facilities and establishing an efficient referral system are essential to improve access for emergency cases and increase the potential impact on maternal mortality.
Keywords: CEmONC; Deliveries; Direct obstetric complications; MSF; Maternal mortality; Newborn; Operational research; SORT IT.
Conflict of interest statement
Permission to carry out the study was obtained from the Institutional Review Board of the Ministry of Public Health, Afghanistan. The study was also approved by the Ethics Advisory Group of the International Union Against Tuberculosis and Lung Disease, Paris, France and the Médecins Sans Frontières (Geneva, Switzerland) Ethics Review Board criteria for studies using routinely collected data. As this was a record review study, informed patient consent was not required.Not applicable.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Tayler-Smith K, Zachariah R, Manzi M, Van den Boogaard W, Nyandwi G, Reid T, Van den Bergh R, De Plecker E, Lambert V, Nicolai M, Goetghebuer S, Christaens B, Ndelema B, Kabangu A, Manirampa J, Harries AD. Achieving the millennium development goal of reducing maternal mortality in rural Africa: an experience from Burundi. Trop Med Int Health. 2013;18:166–174. doi: 10.1111/tmi.12022. - DOI - PubMed
-
- WHO, UNICEF, UNFPA, Bank TW, The United Nations population Division: Trends in Maternal Mortality: 1990–2013. Estimates by WHO, UNICEF, UNIFPA, The World Bank and the United Nations population Division. Geneva: World Health Organisation; 2014.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
