

Early versus newer generation devices for transcatheter aortic valve implantation in routine clinical practice: a propensity score matched analysis
- PMID: 29387427
- PMCID: PMC5786915
- DOI: 10.1136/openhrt-2017-000695
Early versus newer generation devices for transcatheter aortic valve implantation in routine clinical practice: a propensity score matched analysis
Abstract
Aim: Contemporary data comparing early versus newer generation transcatheter heart valve (THV) devices in routine clinical practice are lacking. We sought to compare the safety and efficacy of early versus newer generation THVs in unselected patients undergoing transcatheter aortic valve implantation (TAVI).
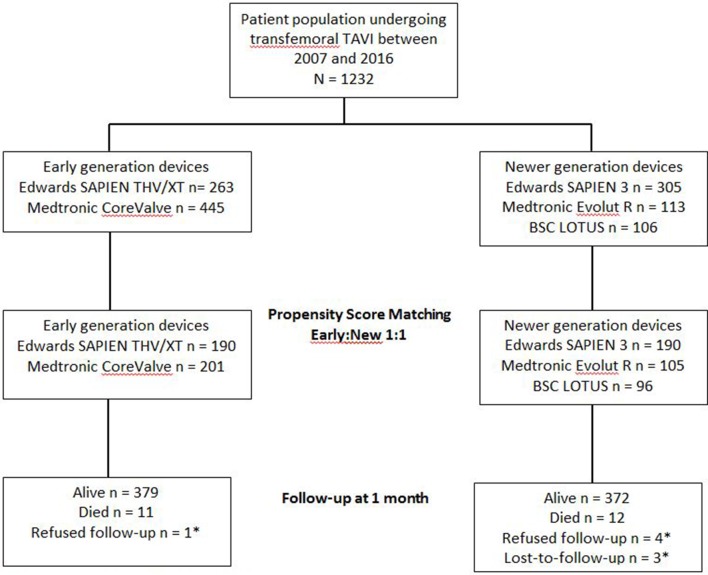
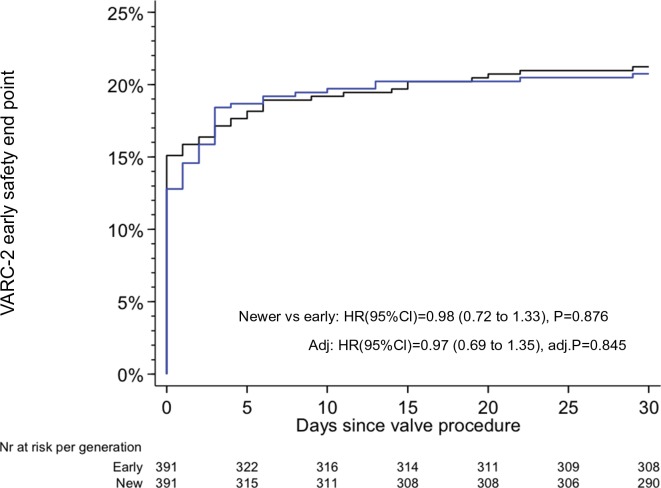
Methods and results: We performed a propensity score matched analysis of patients undergoing transfemoral TAVI at a single centre with early versus newer generation devices between 2007 and 2016. Patients were matched for balloon-expandable versus self-expandable valves and Society of Thoracic Surgeons score. The primary end point was the Valve Academic Research Consortium (VARC)-2 early safety composite end point at 30 days. Among the 391 matched pairs, no differences between early (21.2%) and newer generation (20.8%) THVs regarding the early safety composite end point (HR 0.98, 95% CI 0.72 to 1.33, P=0.88) were observed. The rates of valve embolisation (0.8% vs 4.2%, P=0.005), bleeding events (24.8% vs 32.0%, P=0.028) and moderate-to-severe paravalvular regurgitation (PVR) (3.1% vs 12.1%, P<0.001) were lower among patients receiving newer generation devices. Conversely, patients treated with early generation THVs less frequently experienced annulus rupture (0% vs 2.0%, P=0.008).
Conclusion: Newer compared with early generation THV devices were associated with a lower rate of valve embolisation, PVR and bleeding events.
Keywords: aortic valve disease; valvular disease.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Van Belle E, Juthier F, Susen S, et al. Postprocedural aortic regurgitation in balloon-expandable and self-expandable transcatheter aortic valve replacement procedures: analysis of predictors and impact on long-term mortality: insights from the FRANCE2 Registry. Circulation 2014;129:1415–27. 10.1161/CIRCULATIONAHA.113.002677 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials