

Residual cardiovascular risk in individuals on lipid-lowering treatment: quantifying absolute and relative risk in the community
- PMID: 29387429
- PMCID: PMC5786911
- DOI: 10.1136/openhrt-2017-000722
Residual cardiovascular risk in individuals on lipid-lowering treatment: quantifying absolute and relative risk in the community
Abstract
Objective: The residual cardiovascular disease (CVD) risk in individuals on long-term lipid-lowering treatment (LLT) in the general population is not well described.
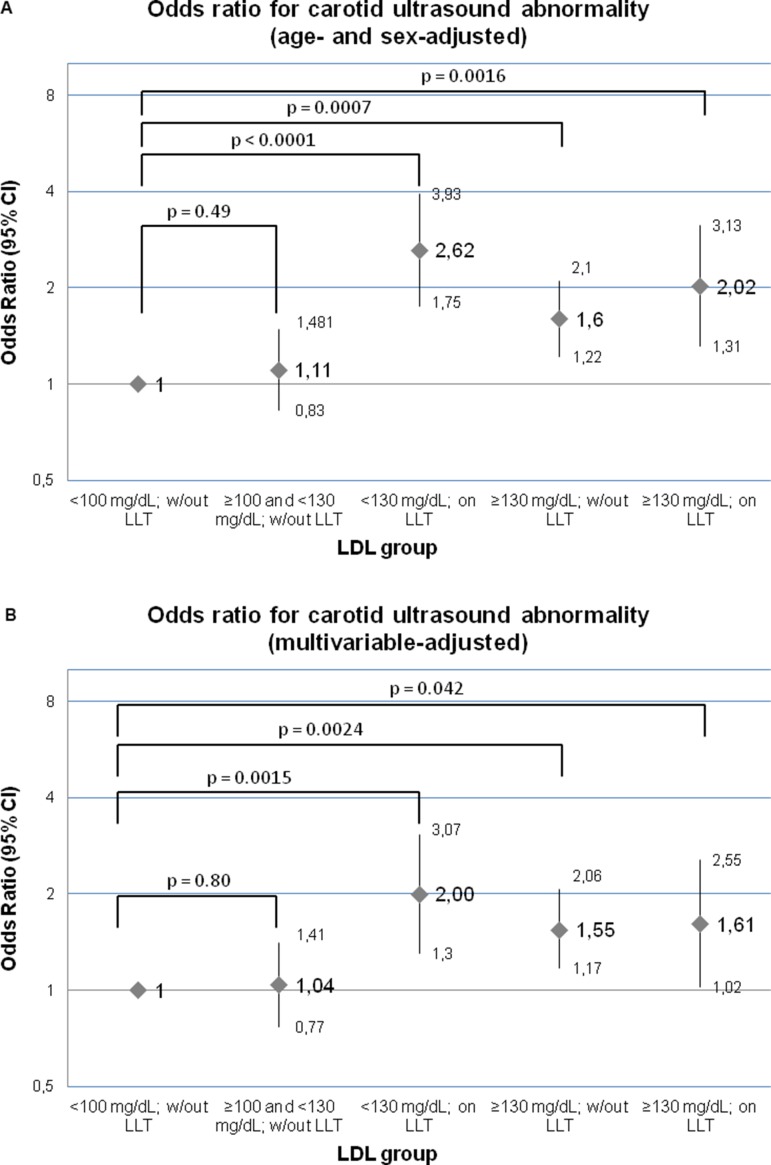
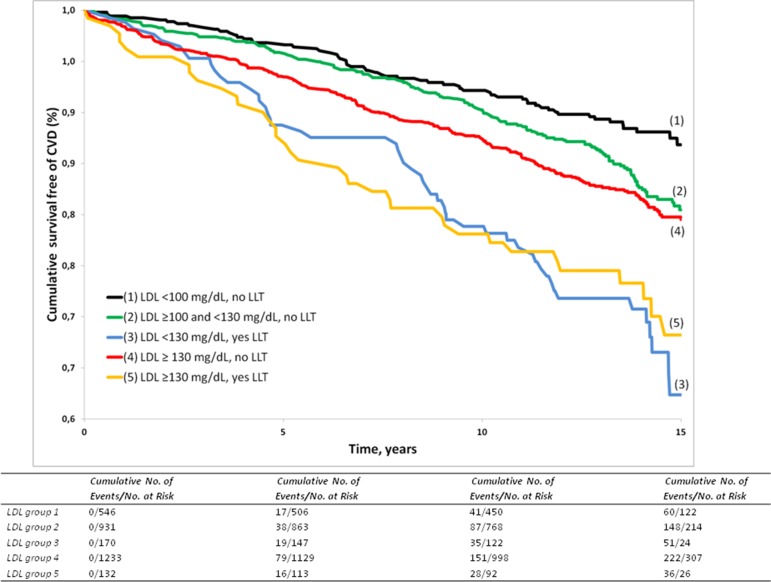
Methods: We estimated absolute CVD risks by age and sex for different categories of low-density lipoprotein cholesterol (LDL-C) levels, stratified by LLT status, and assessed subclinical carotid atherosclerosis in 3012 Framingham Study participants (mean age, 58.4 years; 55% women) free of CVD. Individuals were categorised into five groups: (1) LDL-C <100 mg/dL without LLT; (2) LDL-C ≥100 mg/dL to <130 mg/dL without LLT; (3) LDL-C <130 mg/dL on LLT; (4) LDL-C ≥130 mg/dL without LLT; and (5) LDL-C ≥130 mg/dL on LLT.
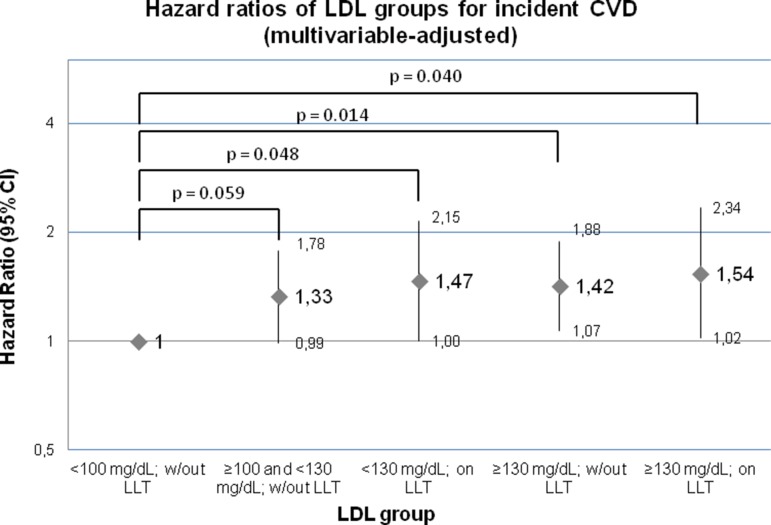
Results: Individuals in groups 3-5 had significantly more carotid atherosclerosis compared with group 1. During follow-up (median, 13.7 years), 548 CVD events occurred. Individuals on LLT (groups 3 and 5) had substantial residual CVD risk (26.7 (95% CI 19.5 to 34.0) and 24.1 (95% CI 16.2 to 31.9) per 1000 person-years, respectively), representing approximately three times the risk for untreated individuals with LDL <100 mg/dL (group 1: 9.0 (95% CI 6.8 to 11.3) per 1000 person-years). Absolute CVD risks rose with age and were slightly greater in men than in women. After adjustment for traditional risk factors, groups 3-5 displayed increased hazards for CVD (HR=1.47, 1.42 and 1.54, respectively) compared with group 1. Further adjustment for carotid atherosclerosis modestly attenuated these results.
Conclusions: There is substantial residual CVD risk in individuals on LLT, compared with participants with optimal LDL-C (<100 mg/dL), even when LDL-C levels <130 mg/dL are reached.
Keywords: LDL; cardiovascular disease; lipids; residual risk; subclinical disease.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Group SSSS. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344:1383–9. - PubMed
-
- Colhoun HM, Betteridge DJ, Durrington PN, et al. Primary prevention of cardiovascular disease with atorvastatin in type 2 diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): multicentre randomised placebo-controlled trial. Lancet 2004;364:685–96. 10.1016/S0140-6736(04)16895-5 - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources