

Optimal antiplatelet strategy after transcatheter aortic valve implantation: a meta-analysis
- PMID: 29387433
- PMCID: PMC5786926
- DOI: 10.1136/openhrt-2017-000748
Optimal antiplatelet strategy after transcatheter aortic valve implantation: a meta-analysis
Abstract
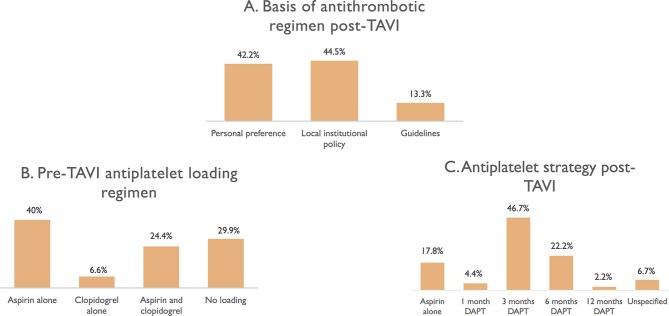
Objective: International guidelines recommend the use of dual antiplatelet therapy (DAPT) after transcatheter aortic valve implantation (TAVI). The recommended duration of DAPT varies between guidelines. In this two-part study, we (1) performed a structured survey of 45 TAVI centres from around the world to determine if there is consensus among clinicians regarding antiplatelet therapy after TAVI; and then (2) performed a systematic review of all suitable studies (randomised controlled trials (RCTs) and registries) to determine if aspirin monotherapy can be used instead of DAPT.
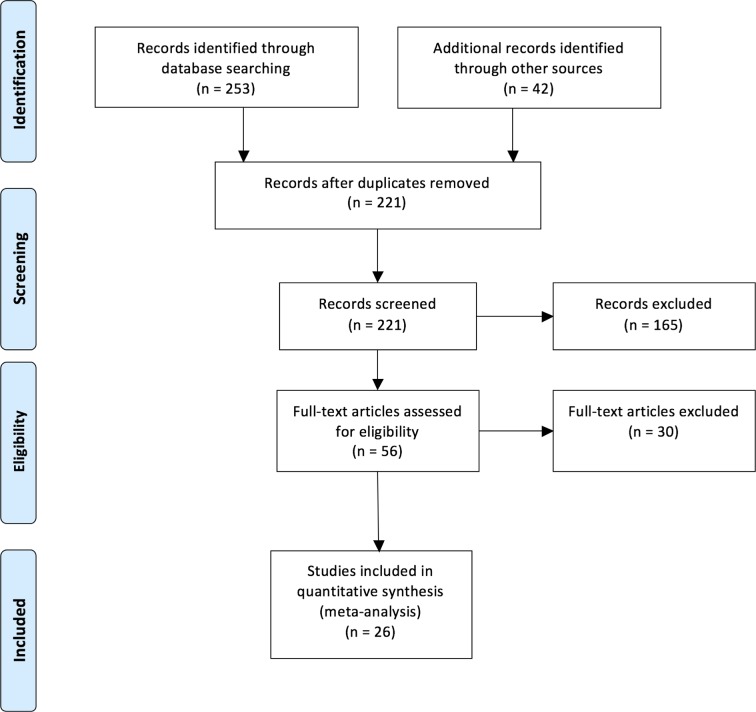
Methods: A structured electronic survey regarding antiplatelet use after TAVI was completed by 45 TAVI centres across Europe, Australasia and the USA. A systematic review of TAVI RCTs and registries was then performed comparing DAPT duration and incidence of stroke, bleeding and death. A variance weighted least squared metaregression was then performed to determine the relationship of antiplatelet therapy and adverse events.
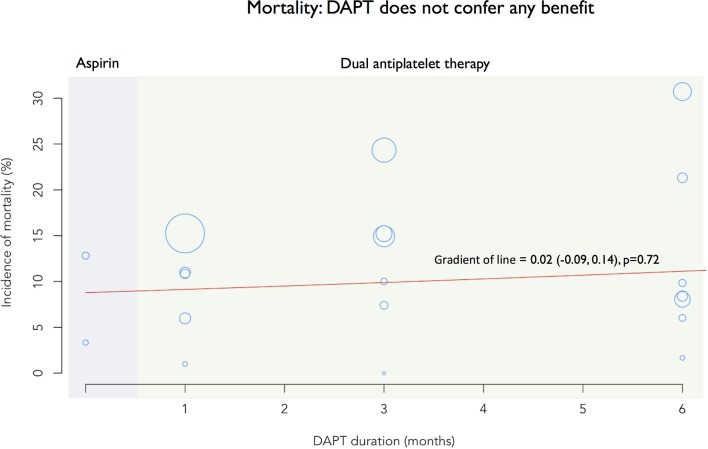
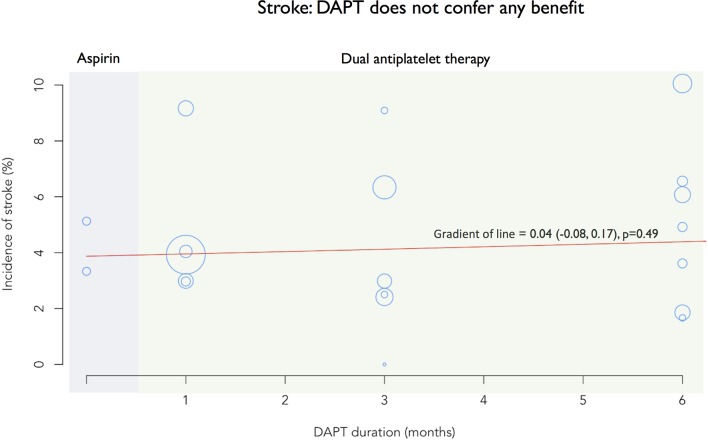
Results: 82.2% of centres routinely used DAPT after TAVI. Median duration was 3 months. 13.3% based their practice on guidelines. 11 781 patients (26 studies) were eligible for the metaregression. There was no benefit of DAPT over aspirin monotherapy for stroke (P=0.49), death (P=0.72) or bleeding (P=0.91).
Discussion: Aspirin monotherapy appears to be as safe and effective as DAPT after TAVI.
Keywords: antiplatelet treatment; aortic valve disease; percutaneous valve therapy; stroke.
Conflict of interest statement
Competing interests: None declared.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources