

Value of surgical resection and timing of therapy in patients with pancreatic cancer at high risk for positive margins
- PMID: 29387477
- PMCID: PMC5786921
- DOI: 10.1136/esmoopen-2017-000282
Value of surgical resection and timing of therapy in patients with pancreatic cancer at high risk for positive margins
Abstract
Background: Surgical resection remains the best chance at long-term survival in pancreatic cancer, though margin-positive resections are associated with diminished survival. We examined the effect of margin-positive resection on survival, as well as the role and timing of additional therapies through the National Cancer Database (NCDB).
Patients and methods: Patients with stage IIA-III pancreatic adenocarcinoma diagnosed from 2004 to 2013 were identified in NCDB. Survival was compared using univariate and multivariate Cox proportional hazards modelling for patients who underwent surgery with negative (R0), microscopically positive (R1) and macroscopically positive (R2) margins or non-surgical treatment. We further analysed patients by margin status, timing of additional therapy (neoadjuvant therapy (NAT) vs adjuvant therapy (AT) vs none) and clinical stage.
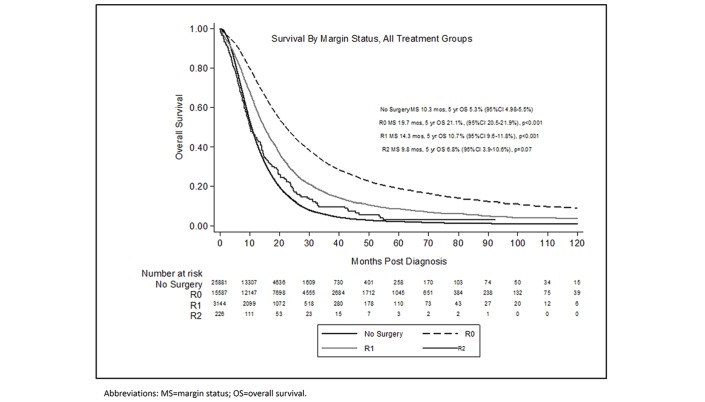
Results: We analysed 44 852 patients. Median survival (MS) for patients who did not undergo surgery was 10.3 months, compared with 19.7 months for R0 (P<0.001), 14.3 months for R1 (P<0.001) and 9.8 months (P=0.07) for R2 resections. NAT (MS 23.2 months) was associated with improved survival compared with AT (MS 21.5 months) in negative-margin patients and equivalent (MS 17.6 months) to AT (MS 16.8 months) in positive-margin patients. Survival for stage III NAT positive-margin patients (MS 19.8 months) was equivalent to AT after negative margins (MS 18.4 months, P=1.00). Improved R0 rates were seen with NAT (88% vs 81%, P<0.001), especially in stage III patients (85% vs 59%, P<0.001).
Conclusion: R1 resections portend poorer survival than R0 but do not negate the benefit of surgery when additional therapy is given. NAT was associated with improved R0 rates and improved survival for stage III positive-margin patients.
Keywords: NCDB; pancreatic cancer; surgical margins.
Conflict of interest statement
Competing interests: None declared.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
