

Psoriasis and inflammatory bowel disease: links and risks
- PMID: 29387596
- PMCID: PMC5683131
- DOI: 10.2147/PTT.S85194
Psoriasis and inflammatory bowel disease: links and risks
Abstract
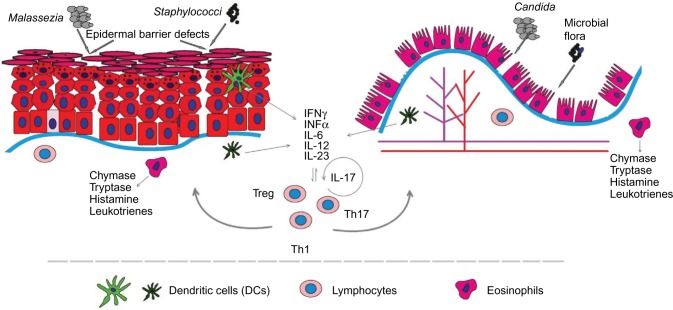
Psoriasis and the spectrum of inflammatory bowel diseases (IBD) are chronic, inflammatory, organotropic conditions. The epidemiologic coexistence of these diseases is corroborated by findings at the level of disease, biogeography, and intrafamilial and intrapatient coincidence. The identification of shared susceptibility loci and DNA polymorphisms has confirmed this correlation at a genetic level. The pathogenesis of both diseases implicates the innate and adaptive segments of the immune system. Increased permeability of the epidermal barrier in skin and intestine underlies the augmented interaction of allergens and pathogens with inflammatory receptors of immune cells. The immune response between psoriasis and IBD is similar and comprises phagocytic, dendritic, and natural killer cell, along with a milieu of cytokines and antimicrobial peptides that stimulate T-cells. The interplay between dendritic cells and Th17 cells appears to be the core dysregulated immune pathway in all these conditions. The distinct similarities in the pathogenesis are also reflected in the wide overlapping of their therapeutic approaches. Small-molecule pharmacologic immunomodulators have been applied, and more recently, biologic treatments that target proinflammatory interleukins have been introduced or are currently being evaluated. However, the fact that some treatments are quite selective for either skin or gut conditions also highlights their crucial pathophysiologic differences. In the present review, a comprehensive comparison of risk factors, pathogenesis links, and therapeutic strategies for psoriasis and IBD is presented. Specific emphasis is placed on the role of the immune cell species and inflammatory mediators participating in the pathogenesis of these diseases.
Keywords: Crohn’s disease; immune cells; inflammation; inflammatory bowel disease; psoriasis; ulcerative colitis.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
References
-
- Nestle FO, Kaplan DH, Barker J. Psoriasis. N Engl J Med. 2009;361(5):496–509. - PubMed
-
- Baumgart DC, Sandborn WJ. Inflammatory bowel disease: clinical aspects and established and evolving therapies. Lancet. 2007;369:1641–1657. - PubMed
-
- Lolli E, Saraceno R, Calabrese E, et al. Psoriasis phenotype in inflammatory bowel disease: a case-control prospective study. J Crohns Colitis. 2015;9(9):699–707. - PubMed
-
- Molodecky NA, Soon IS, Rabi DM, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142:46–54. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
