

Outpatient Worsening Heart Failure as a Target for Therapy: A Review
- PMID: 29387880
- PMCID: PMC7474527
- DOI: 10.1001/jamacardio.2017.5250
Outpatient Worsening Heart Failure as a Target for Therapy: A Review
Abstract
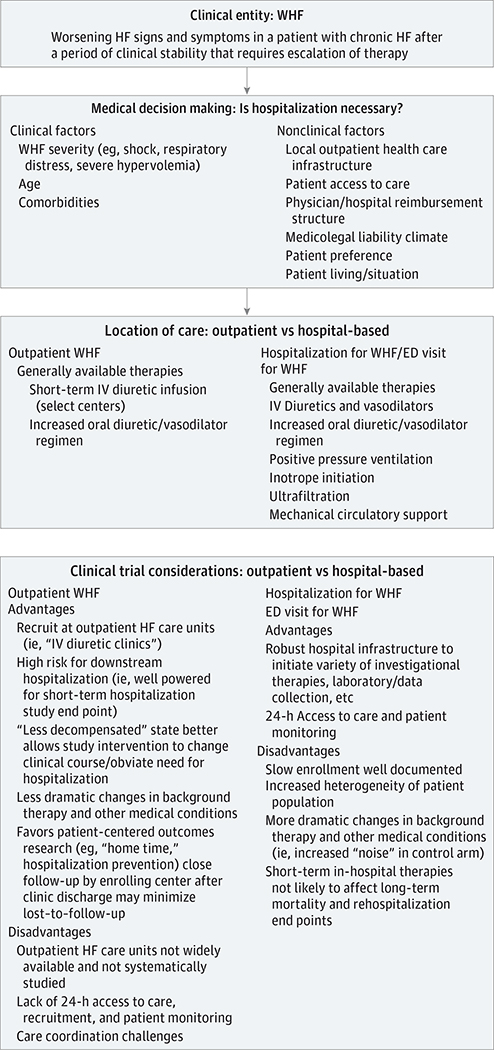
Importance: Hospitalizations for worsening heart failure (WHF) represent an enormous public health and financial burden, with physicians, health systems, and payers placing increasing emphasis on hospitalization prevention. In addition, maximizing time out of the hospital is an important patient-centered outcome. In this review, we discuss the concept of outpatient WHF, highlight the rationale and data for the outpatient treatment of WHF as an alternative to hospitalization, and examine opportunities and strategies for developing outpatient "interceptive" therapies for treatment of worsening symptoms and prevention of hospitalization.
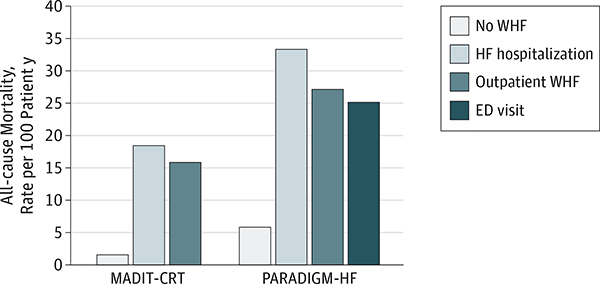
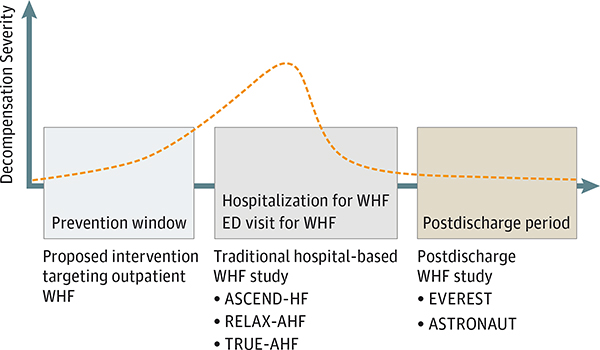
Observations: Worsening heart failure has traditionally been synonymous with an episode of in-hospital care for worsening symptoms. While WHF often leads to hospitalization, many patients experience WHF in the outpatient setting and carry a similarly poor prognosis. These findings support WHF as a distinct condition, independent of location of care. For those that are hospitalized, most patients have an uncomplicated clinical course, with diuretics as the only intravenous therapy. Although complicated scenarios exist, it is conceivable that improved tools for outpatient management of clinical congestion would allow a greater proportion of hospitalized patients to receive comparable care outside the hospital. Most patients with WHF have a gradual onset of congestive signs and symptoms, offering a potential window in which effective therapy may abort continued worsening and obviate the need for hospitalization. To date, outpatient WHF has received minimal attention in randomized clinical trials, but this high-risk group possesses key features that favor effective clinical trial investigation.
Conclusions and relevance: As the public health and economic burdens of heart failure continue to grow, recognizing the entity of outpatient WHF is critical. Efforts to reduce heart failure hospitalization should include developing effective therapies and care strategies for outpatient WHF. The outpatient WHF population represents a major opportunity for therapeutic advancements that could fundamentally change heart failure care delivery.
Figures
References
-
- Setoguchi S, Stevenson LW, Schneeweiss S. Repeated hospitalizations predict mortality in the community population with heart failure. Am Heart J. 2007;154(2):260–266. - PubMed
-
- Nieminen MS, Dickstein K, Fonseca C, et al. The patient perspective: quality of life in advanced heart failure with frequent hospitalisations. Int J Cardiol. 2015;191:256–264. - PubMed
-
- Nieminen MS, Brutsaert D, Dickstein K, et al.; EuroHeart Survey Investigators; Heart Failure Association, European Society of Cardiology. EuroHeart Failure Survey II (EHFSII): a survey on hospitalized acute heart failure patients: description of population. Eur Heart J. 2006;27 (22):2725–2736. - PubMed
-
- Zile MR, Bennett TD, St John Sutton M, et al. Transition from chronic compensated to acute decompensated heart failure: pathophysiological insights obtained from continuous monitoring of intracardiac pressures. Circulation. 2008;118(14): 1433–1441. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
