

Melioidosis
- PMID: 29388572
- PMCID: PMC6456913
- DOI: 10.1038/nrdp.2017.107
Melioidosis
Abstract
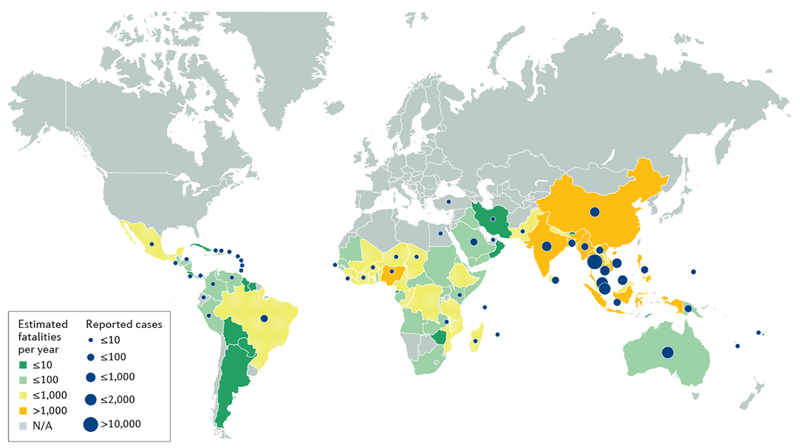
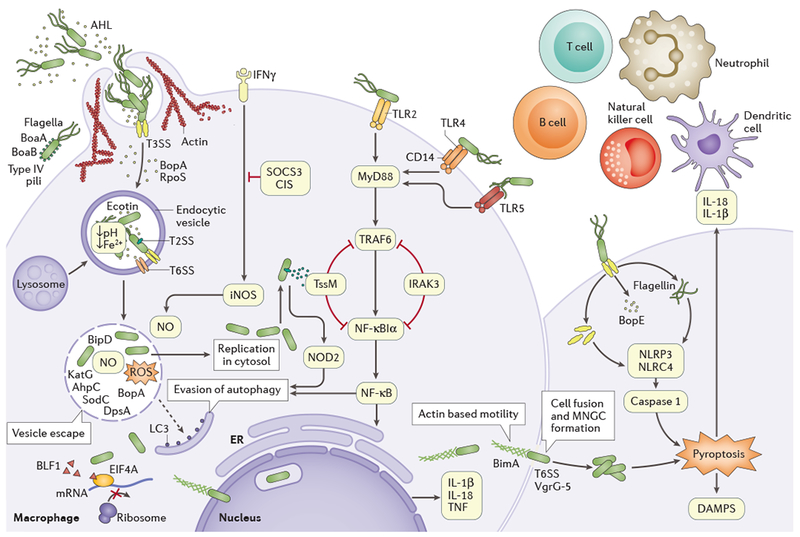
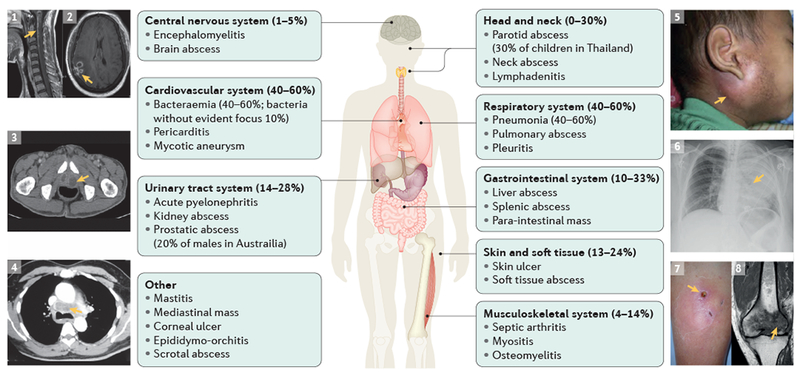
Burkholderia pseudomallei is a Gram-negative environmental bacterium and the aetiological agent of melioidosis, a life-threatening infection that is estimated to account for ∼89,000 deaths per year worldwide. Diabetes mellitus is a major risk factor for melioidosis, and the global diabetes pandemic could increase the number of fatalities caused by melioidosis. Melioidosis is endemic across tropical areas, especially in southeast Asia and northern Australia. Disease manifestations can range from acute septicaemia to chronic infection, as the facultative intracellular lifestyle and virulence factors of B. pseudomallei promote survival and persistence of the pathogen within a broad range of cells, and the bacteria can manipulate the host's immune responses and signalling pathways to escape surveillance. The majority of patients present with sepsis, but specific clinical presentations and their severity vary depending on the route of bacterial entry (skin penetration, inhalation or ingestion), host immune function and bacterial strain and load. Diagnosis is based on clinical and epidemiological features as well as bacterial culture. Treatment requires long-term intravenous and oral antibiotic courses. Delays in treatment due to difficulties in clinical recognition and laboratory diagnosis often lead to poor outcomes and mortality can exceed 40% in some regions. Research into B. pseudomallei is increasing, owing to the biothreat potential of this pathogen and increasing awareness of the disease and its burden; however, better diagnostic tests are needed to improve early confirmation of diagnosis, which would enable better therapeutic efficacy and survival.
Conflict of interest statement
Competing interests statement
D.A.B.D. acted as a consultant to Soligenix, Inc. All other authors declare no competing interests.
Figures
References
-
- Limmathurotsakul D et al. Predicted global distribution of Burkholderia pseudomallei and burden of melioidosis. Nat. Microbiol 1, 15008 (2016). - PubMed
-
This is a key publication on the global burden of melioidosis that uses human, animal and environmental data to estimate the number of human melioidosis cases per year at 165,000 worldwide, of which 89,000 are fatal.
-
- Wiersinga WJ, Currie BJ & Peacock SJ Melioidosis. N. Engl. J. Med 367, 1035–1044 (2012). - PubMed
-
This article reviews the clinical manifestations, epidemiology, pathogenesis, diagnosis and treatment of melioidosis, with an emphasis on clinical management.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
