

Worsening renal function definition is insufficient for evaluating acute renal failure in acute heart failure
- PMID: 29388735
- PMCID: PMC5933958
- DOI: 10.1002/ehf2.12264
Worsening renal function definition is insufficient for evaluating acute renal failure in acute heart failure
Abstract
Aims: Whether or not the definition of a worsening renal function (WRF) is adequate for the evaluation of acute renal failure in patients with acute heart failure is unclear.
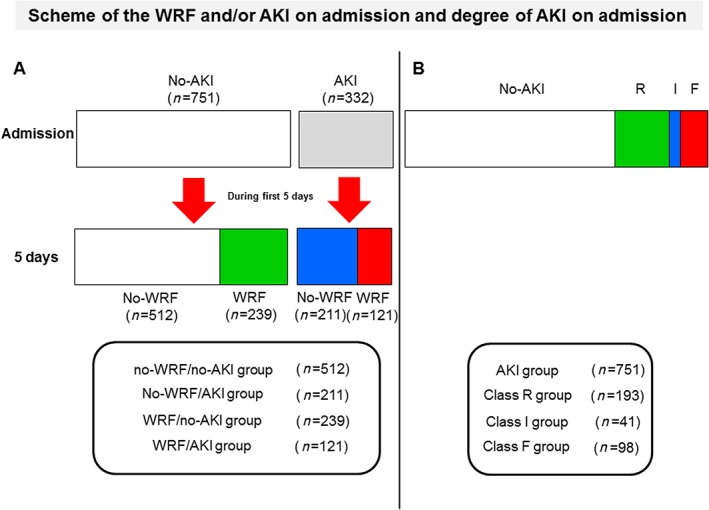
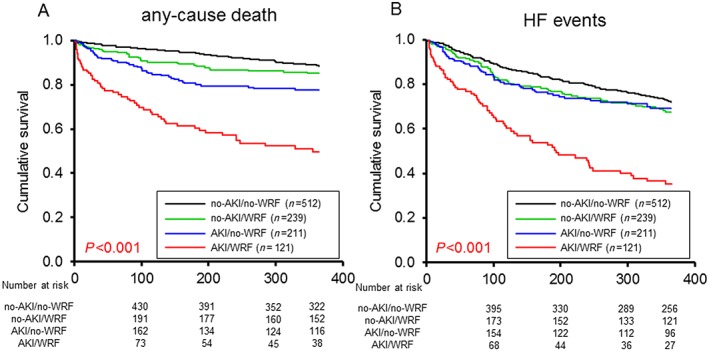
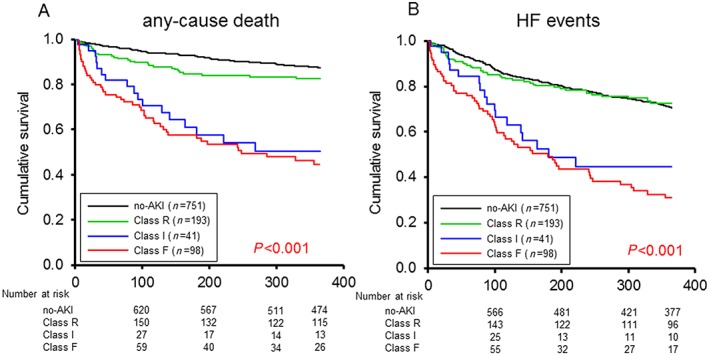
Methods and results: One thousand and eighty-three patients with acute heart failure were analysed. A WRF, indicated by a change in serum creatinine ≥0.3 mg/mL during the first 5 days, occurred in 360 patients while no-WRF, indicated by a change <0.3 mg/dL, in 723 patients. Acute kidney injury (AKI) upon admission was defined based on the ratio of the serum creatinine value recorded on admission to the baseline creatinine value and placed into groups based on the degree of AKI: no-AKI (n = 751), Class R (risk; n = 193), Class I (injury; n = 41), or Class F (failure; n = 98). The patients were assigned to another set of four groups: no-WRF/no-AKI (n = 512), no-WRF/AKI (n = 211), WRF/no-AKI (n = 239), and WRF/AKI (n = 121). A multivariate logistic regression model found that no-WRF/AKI and WRF/AKI were independently associated with 365 day mortality (hazard ratio: 1.916; 95% confidence interval: 1.234-2.974 and hazard ratio: 3.622; 95% confidence interval: 2.332-5.624). Kaplan-Meier survival curves showed that the rate of any-cause death during 1 year was significantly poorer in the no-WRF/AKI and WRF/AKI groups than in the WRF/no-AKI and no-WRF/no-AKI groups and in Class I and Class F than in Class R and the no-AKI group.
Conclusions: The presence of AKI on admission, especially Class I and Class F status, is associated with a poor prognosis despite the lack of a WRF within the first 5 days. The prognostic ability of AKI on admission may be superior to WRF within the first 5 days.
Keywords: Acute decompensated heart failure; Acute kidney injury; Acute renal failure; Cardio renal syndrome; RIFLE criteria.
© 2018 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Figures
References
-
- Forman DE, Butler J, Wang Y, Abraham WT, O'Connor CM, Gottlieb SS, Loh E, Massie BM, Rich MW, Stevenson LW, Young JB, Krumholz HM. Incidence, predictors at admission, and impact of worsening renal function among patients hospitalized with heart failure. J Am Coll Cardiol 2004; 43: 61–67. - PubMed
-
- Núñez J, Miñana G, Santas E, Bertomeu‐González V. Cardiorenal syndrome in acute heart failure: revisiting paradigms. Rev Esp Cardiol 2015; 68: 426–435. - PubMed
-
- Bellomo R, Kellum JA, Ronco C. Defining and classifying acute renal failure: from advocacy to consensus and validation of the RIFLE criteria. Intensive Care Med 2007; 33: 409–413. - PubMed
-
- Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P, Acute Dialysis Quality Initiative workgroup . Acute renal failure – definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care 2004; 8: R204–R212. - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical